Abstract –
The objectives of this study were to determine the importance of diagnostic laparoscopy for the accurate diagnosis of endometriosis and to correlate the findings with infertility. Participants in this study included 336 women who were 18–45 years old, had no past medical history of abdominal operations, and complained of chronic symptoms of pelvic pain. In all these cases there were no pathological pelvic ultrasound findings. Also, nongynaecological diseases where excluded. Diagnostic laparoscopy was performed in all patients. In 191 women (56.8%) no pathology was found during the diagnostic laparoscopy, and 89 women (26.4%) actually reported improvement or even complete cure from their symptoms after the operation. In the majority of pathological cases the laparoscopy revealed various stages of endometriosis (n = 101; 30%). Other gynecological causes which were diagnosed during the laparoscopy where pelvic adhesions due to inflammatory disease (n = 37; 11%), ovarian cysts (n = 5; 1.5%), and uterine fibroids (n = 2; 0.5%). Diagnostic laparoscopy is the most accurate method for excluding the pathology related with chronic pelvic pain. Endometriosis seems to be responsible for the majority of pathological cases. Almost 60% of women have no pathology when examined with laparoscopy. A high percentage of symptoms can be phycogenic.
Introduction –
Endometriosis is defined as the presence of endometrial-like tissue outside the uterus, which induces a chronic, inflammatory reaction. While a number of theories have been proposed for the pathogenesis of endometriosis, that of retrograde menstruation is the most popular and plausible. Retrograde menstruation is common and is seen in 75–90% of women who have had laparoscopies at the time of menstruation [1]. Menstrual blood does not always contain endometrial cells and the factors that influence implantation of ectopic endometrium are uncertain, for the prevalence of endometriosis has been estimated as 1–20%. Women with endometriosis appear to have altered immune function, which may permit implantation of regurgitated endometrium. Most endometriotic lesions have the classic blue/black pigmented appearance. Atypical lesions could be similar to blisters, white plaques, nodules, and peritoneal defects [2, 3]. It has been suggested that nonpigmented lesions are more common in younger women and that darker lesions represent older disease [4].
The associated symptoms can impact on general physical, mental, and social well being. However, women may not have any symptoms at all. Laparoscopy is the mainstay of diagnosis and classification of endometriosis. All classification systems for endometriosis are subjective and correlate poorly with pain symptoms but may be of value in infertility prognosis and management.
Materials and methods –
This retrospective study included 336 women who were 18–45 years old. The women in our study group had no past medical history of abdominal operations and all of them complained of symptoms of chronic pelvic pain. The duration of symptoms was at least 6 months in order to be characterized as chronic. Of these women, 106 were also referred for primary or secondary infertility. In all these cases, gynaecological examination and transvaginal pelvic ultrasound were performed. There were no pathological pelvic ultrasound findings. Also, nongynaecological diseases were excluded. Diagnostic laparoscopy was performed in all these women by four different consultant obstetricians gynaecologists.
Results –
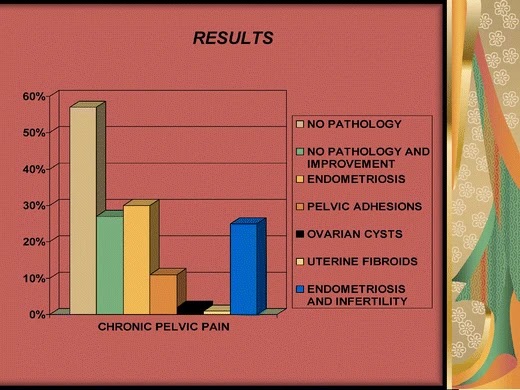
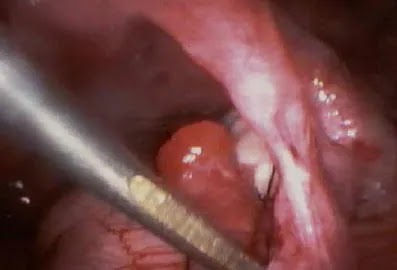
In 191 women (56.8%) no pathology was found during the diagnostic laparoscopy, and 89 women (26.4%) actually reported improvement or even complete cure from their symptoms after the operation. In the majority of pathological cases the laparoscopy revealed various stages of endometriosis (n = 101; 30%) that was diagnosed during the procedure on observation of the lesions and, in cases of endometriomas, also by histopathology report. For the women with endometriosis, almost 85% (n = 84) complained of primary or secondary infertility. Other gynecological causes which were identified with laparoscopy were pelvic adhesions due to inflammatory disease (n = 37; 11%), ovarian cysts (n = 5; 1.5%), and uterine fibroids (n = 2; 0.5%). No pathology was found in 16 (15%) women with primary or secondary infertility. The cause for infertility in 6 (5.5%) women was pelvic adhesions due to inflammatory disease. Endometriosis accounted for 80% (n = 84) of infertility cases (Figs.1).
Discussion –
It is well known that the degree of endometriosis does not correlate with symptomatology: pelvic pain, dyspareunia, and dysmenorrhea. Moreover, it is not possible to predict which patients will develop progressive disease with resultant pelvic adhesions and ovarian cysts. Finding endometriosis may be coincidental in some women [5]. Careful laparoscopic assessment of the pelvis reveals signs of endometriosis in up to 18% of women with proven fertility [6]. For a definitive diagnosis of endometriosis, visual inspection of the pelvis at laparoscopy is the gold standard investigation unless disease is visible in the posterior vaginal fornix or elsewhere [5]. A meta-analysis against a histological diagnosis showed that a positive laparoscopic examination increases the likelihood of detecting the disease to 32% (95% CI; range, 21–46%) and a negative laparoscopy decreases the likelihood to 0.7% (95% CI; range, 0.1–5%) [7]. There is insufficient evidence to justify scheduling the laparoscopy for a specific time in the menstrual cycle, but it should not be performed during or within 3 months of hormonal treatment to avoid underdiagnosis [8, 9]. At laparoscopy, deeply infiltrating endometriosis may have the appearance of minimal disease, resulting in an underestimation of disease severity [10]. Positive histology confirms the diagnosis of endometriosis; negative histology does not exclude it. Visual inspection is usually adequate but histological confirmation of at least one lesion is ideal. In cases of ovarian endometrioma and in deeply infiltrating disease, histology should be obtained to identify endometriosis and to exclude rare instances of malignancy.
Laparoscopy is the gold standard diagnostic test in clinical practice for the accurate diagnosis of endometriosis [5]. Compared with laparoscopy, transvaginal ultrasound (TVS) has limited value in diagnosing peritoneal endometriosis, but it is a useful tool to make or exclude the diagnosis of an ovarian endometrioma [11]. At present, there is insufficient evidence to indicate that magnetic resonance imaging (MRI) is a useful test to diagnose or exclude endometriosis compared to laparoscopy [5]. A number of markers for endometriosis have been proposed, and probably the most commonly used is the glycoprotein CA-125, an oncofetal celomic epithelium differentiation antigen. It has been suggested that 35 U/ml could be used as a cut-off serum concentration for CA-125, below which endometriosis is unlikely to be present. Unfortunately CA-125 measurements do not correlate well with either the progression of the disease or the response of endometriosis to treatment. Compared with laparoscopy, measuring serum levels of CA-125 has no value as a diagnostic tool. The test’s performance in diagnosing all disease stages is limited, since it has about 28% sensitivity [12]. The test’s performance for moderate to severe endometriosis is a bit better with a sensitivity reaching 47% [12].
There is still debate about the extent to which endometriosis affects fertility in the absence of pelvic deformity. It has been suggested that the peritoneal environment is altered with interference to the sperm motility, to the oocyte pick-up by the fallopian tube, and to fertilization. Fertility can also be impaired due to dyspareunia caused by endometriosis. It is easy to assume that severe endometriosis can affect fertility by distorting pelvic anatomy with adhesions [13, 14]. The effect of endometriosis on assisted conception therapy results is unclear. According to HFEA (Human Fertilization and Embryology Authority), there is no difference in pregnancy rates in patients with endometriosis, without taking into account the stage of endometriosis [15]. Other authors insist that the fertilization rate, pregnancy rate (PR) per transfer, and birth rate were significantly lower in patients with severe endometriosis (stages III and IV) in comparison with patients with tubal infertility [16].
In almost 50–60% of cases with chronic pelvic pain symptoms, no organic cause is found during laparoscopy [17, 18]. In fact, it may be even more difficult to differentiate the organic from psychogenic pain in patients with symptoms lasting more than 6 months. Whatever the original cause of the chronic pelvic pain, it is quite likely that other facts, mainly psychological, could maintain or exacerbate the symptoms. Patients with chronic pelvic pain are more often found to suffer from depression and somatization disorders. These facts could explain that in a significant percentage of patients, although no organic pathology is found, there is improvement or even cure from the symptoms after a diagnostic laparoscopy [17, 19].
According to our study 85% of women with endometriosis also had infertility problems, and endometriosis accounted for almost 80% of all infertility cases. Of all patients, 30% reported chronic pelvic pain due to endometriosis, and in only 16 of 101 (16%) women with endometriosis no fertility problems were found.
Conclusions – Diagnostic laparoscopy is the most accurate method for excluding the pathology related to chronic pelvic pain. Endometriosis seems to be responsible for most pathological cases of chronic pelvic pain and also for the highest percentage of cases who are referred with primary and secondary infertility. Almost 60% of women with symptoms of chronic pelvic pain have no pathology when examined with laparoscopy.
Source – https://gynecolsurg.springeropen.com/articles/10.1007/s10397-007-0357-7
Mohak infertility center is the top leading Best fertility hospital in india, Dr. Shilpa Bhandari is one of the best IVF specialist in indore at Mohak infertility center. providing best IVF treatments, test tube baby treatment and infertility treatment in Indore at an affordable IVF cost in indore. for more info touch with us. Book an appointment Call now 7898047572 For more information, visit – https://www.mohakivf.com
Please go through our social media :
like our page to no more about ivf
Facebook : https://www.facebook.com/MOHAK-IVF-1167147806785287/
Please do follow on Instagram
Instagram : https://www.instagram.com/mohak_ivf/
To More Post: Failed IVF: Not an end to life