Infertility is defined as the inability to conceive within 12 months. If you are infertile, then you cannot get pregnant naturally and have children Approximately 85% of couples will achieve pregnancy within one year of trying, with the greatest likelihood of conception occurring during the earlier months. Additional 7% of couples will conceive in the second year and the couples who are enable to conceive even after trying this long defined as infertile . Until recently, it was usually the women who were assumed to be the origin of any fertility issues. However, recent studies as conducted by the International Committee for Monitoring Assisted Reproductive Technology, World Health Organization, show that nearly 50% of infertility is related to the reproductive anomalies or disorders in the male.
WHAT IS REQUIRED FOR A COUPLE TO BECOME PREGNANT:
In order for a couple to become pregnant, at least four things have to happen:
OVULATION -A woman must produce and release a healthy egg from one of her ovaries.This is known as ovulation.
FERTILIZATION-A man must produce viable sperm which can successfully fertilize the woman’s egg. This procedure is known as fertilization.
TRANSPORTATION-The egg must travel through a fallopian tube toward the uterus.
MPLANTATION-The fertilized egg must attach to the inside of the uterus.
What are the causes of low sperm count or abnormal sperm function in men?
Low sperm count or abnormal sperm function may be caused by:
Undescended testicles
If there is any Genetic defects/DNA damage
When a man is suffering from Diabetes
If a man had a Prior bacterial or viral infections such as mumps or adenovirus
Had a history of trauma or prior surgeries on the testicles or inguinal region
If a person has enlarged veins (varicoceles) in the testes that can increase blood flow and heat, both of which affect the number and shape of the sperm
If a man is exposed to chemicals like pesticides, radiation, and chemotherapy
If a man is an Alcohol user, marijuana user, and uses tobacco smoke
If a man is on Steroid
There is overexposure to heat (such as in saunas and hot tubs)
If surgical removal of one of the testicles due to cancer
In addition, there can be problems with the delivery of sperm and subsequent fertilization due to any of the following:
Premature ejaculation
Damage or injury to the reproductive organs
Semen entering the bladder instead of emerging through the penis during orgasm (retrograde ejaculation)
Certain genetic diseases (such as cystic fibrosis)
Men who have previously had a vasectomy and wish to father a child have two choices. They either need to have the vasectomy reversed or have sperm retrieved through a surgical procedure as part of assisted reproductive techniques.
What are the causes of infertility in women?
The causes of infertility in women can include many of the following:
Hormonal issues: These can be due to the lack of the necessary synchronized hormonal changes leading to the release of an egg from the ovary.
Disorders of the thyroid gland: Either too much thyroid hormone or too little thyroid hormone can interfere with the menstrual cycle or cause infertility
Gland disorders: These hormonal disorders may include polycystic ovarian syndrome (PCOS), or problems with the hypothalamus, pituitary gland, adrenal gland (such as Cushing’s syndrome or congenital adrenal hyperplasia)
Structural issues: Benign growths (such as polyps and fibroids) in the uterus, blocked fallopian tubes, abnormal anatomy of the cervix or uterus, endometriosis, scar tissue
Fallopian tube damage can include scarring from prior surgery and/or pelvic infections. These include pelvic inflammatory disease (PID). Problems with transportation of the egg(s) can occur due to damaged or blocked fallopian tubes.
Diminished ovarian reserve, premature menopause or cessation of ovulation (primary ovarian insufficiency); changes in egg quality or quantity can affect fertility
Additional factors:
Poor diet that is lacking in nutrients
Athletic overtraining
Stress
Too much exposure to certain chemicals and toxins (for example, tobacco smoke, alcohol, marijuana, pesticides, radiation, and chemotherapy)
Certain medications (the effect usually is temporary)
Sickle cell disease
Kidney disease
Celiac disease
Diabetes
Women who have had a tubal ligation or an Essure® device (forms of permanent birth control) should speak with a gynecologist about their options.
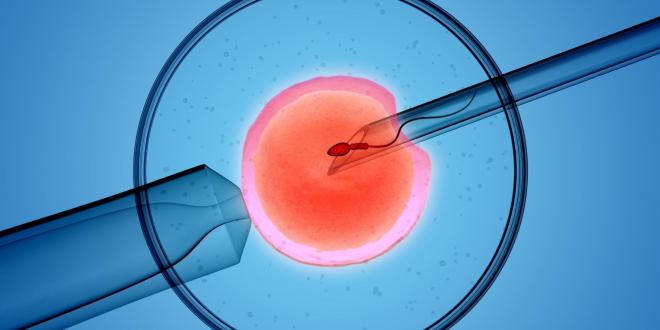
It is a process of fertilisation where an egg is combined with sperm outside the body, is known to be in vitro fertilization.
Procedure in short include-
monitoring and stimulating a woman’s ovulatory process, removing an ovum or ova (egg or eggs) from the woman’s ovaries and letting sperm fertilise them in a liquid in a laboratory. After the fertilised egg (zygote) undergoes embryo culture for 2–6 days, it is implanted in the same or another woman’s uterus, with the intention of establishing a successful pregnancy.
Sometimes question arises that Can a female get pregnant after her reproductive year or after menopause?
The reply to this question is yes, a female can be pregnant after her reproductive year by the help of In vitro fertilization.
With egg donation and IVF, women who are past their reproductive years, have infertile male partners, have fertility issues, or have reached menopause can still become pregnant.
Risk of IVF over age 40
Although all the pregnancies can be risky, but there are greater risk for women who are older and are over the age of 40. The older the women the riskier the pregnancy. As women get older, they are more likely to suffer from conditions such as gestational diabetes and pre-eclampsia. If older women do conceive over the age of 40, their offspring may be of lower birth weight, and more likely to requires intensive care.
Complications during IVF treatment are as following :
Multiple pregnancies, which increases the risk of low birth weight and premature birth
Miscarriage (pregnancy loss)
Ectopic pregnancy (when the eggs implant outside the uterus)
ovarian hyper stimulation syndrome (OHSS), a rare condition involving an excess of fluid in the abdomen and chest
Bleeding, infection, or damage to the bowels or bladder (rare)
Some symptoms while IVF which should not be ignored are:
Endometriosis: Endometriosis is a riot that grows the endometrial cells which form the inside of the uterus but in a position outside of the uterus. The inside layer of your uterus is called the endometrial. The accurate reason for endometriosis has not been acknowledged. Endometrial tissue is shack each month throughout menstruation.
Endometriosis is most frequently found on your bowel, ovaries, Fallopian tubes, and the surface of the uterus and the membrane lining of the pelvic cavity. Endometrial tissue growing outer surface of your uterus is known as an endometrial implant. Endometriosis is less commonly originated to engross the cervix, bladder, and vagina. Infrequently, endometriosis occurs in the outer surface of the pelvis.
Stages of Endometriosis:
Endometriosis is defined in four stages that are I-minimal, II-mild, III-moderate, and IV-severe. It is based on the precise place, level, and profundity of the endometriosis implants with the presence and harshness of blemish tissue. The stage of endometriosis is not interrelated to the degree of warning signs a woman experiences, but sterility is frequent with stage IV endometriosis.
Signs and Symptoms of Endometriosis:
Following are the signs and symptoms that can be shown in women who have endometriosis:
Pain (frequently pelvic) that generally occurs just before menstruation and lessens after menstruation
Sore sexual interaction
Contraction during intercourse
Cramping or pain during bowel activities or urination
Infertility
Pain with pelvic examinations
Other symptoms that can be related to endometriosis:
• Lower abdominal pain, • diarrhea and/or constipation, • Low back pain, • Chronic fatigue • Uneven or heavy menstruation, • Painful urination, or • Bloody urine (predominantly during menstruation)
Risk Factor of Endometriosis:
About 2 to 10 percent of procreation women in the US between the ages of 25-40 have endometriosis. It frequently expands years after the start of your menstrual cycle. This condition can be excruciating but you should understand the risk factors that can assist you to conclude whether you’re vulnerable to this situation and when you should talk to your doctor or else.
Causes of Endometriosis:
Even though the accurate reason for endometriosis is not assured, likely explanations embrace:
• Retrospective menstruation • Revolution of peritoneal cells • Emergent cell transformation • Surgical blemish implantation • Endometrial cell transport • Resistant system chaos
Treatment for endometriosis:
Endometriosis can be delighted with medications and/or surgery. The goals of endometriosis treatment may include symptom relief and/or augmentation of fertility.
Mohak Infertility Center Indore is a one of the Best infertility hospitals and Best IVF centers in MP, which treats IVF, IUI, ICSI and infertility treatment in Indore. Mohak Infertility Center is known for the most successful IVF treatment in Indore. Her dream is to provide affordable, honest patient care to couple seeking to enhance their families. If you are also looking for the Best IVF specialist and Best centre for IVF in Indore, then contact Mohak Infertility Center. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com
Over the years, IVF has turned out to be a blessing for married couples facing fertility issues. Major reasons for couples being infertile can be: –
1. Polycystic Ovary Syndrome(PCOS) 2. Uterine Fibroids 3. Male Infertility 4. Fallopian Tube Damage 5. Reduced Fertility in women after the age of 40
This is where IVF (In-Vitro Fertilization) comes to rescue. In this process, women’s eggs are retrieved from ovaries and then fertilized with sperm. The fertilized egg is called an embryo. The embryo can be frozen for storage or be transferred to the female’s uterus. The embryo then develops in the womb to become a baby.
IVF might include any of the 5 situations: –
1. Wife’s egg and husband’s sperm2. Wife’s egg and donor’s sperm3. Donor’s egg and husband’s sperm4. Donor’s egg and donor’s sperm5. Donated Embryo
Wife’s egg and husband’s sperm
Wife’s egg and donor’s sperm
Donor’s egg and husband’s sperm
Donor’s egg and donor’s sperm
Donated Embryo
Initially, before IVF process, women undergo OVARIAN RESERVE TESTING. This test is done to check for the level of follicle stimulating hormone (FSH).
Men also go through the test to check for the quality of their sperms. If the sperms are deformed or damaged, ICSI (intracytoplasmic sperm injection) is injected in the eggs of female. This process also comes under the IVF.
Knowing about IVF process is as important as knowing about the best IVF centers in your region.
There are plenty of things that need to be looked carefully while looking for an IVF centre. This is important to avoid any kind of future medical complications. We are enumerating some tips to take care while choosing your IVF centre: –
Any fertility clinic is as good as its doctors. If the medical specialists do not seem authentic and trustworthy with their answers, it’s better to search for the better one. It’s also important to look for the IVF Centre’s affiliations.
While looking for a better facility, do ask for their CDC reports. It tells us about hospital’s success rate over the years.
Since IVF does not come under any insurance cover, this might be problematic for some couples who have financial constraints. So ask for every single penny detail that the IVF process demands.
There ‘s no doubt that the experienced IVF centers will be helpful in avoiding miscarriage, multiple pregnancies, bleeding, infection or any damage to the bladder.
One of the best IVF centers in Indore for IVF operation is Mohak Infertility Centre. Over the years, Mohak IVF center has maintained a high success rate with their patients. Mohak IVF has blessed many sterile couples with baby squeals. So, if you’re a couple struggling with infertility problem, then contact Mohak Infertility Centre for test-tube baby, surrogacy and pregnancy.
Mohak Infertility Centre is a one of the best infertility treatment hospitals and Test tube baby centers in Indore. We provide the world class IUI, IVF treatment, ICSI treatment, test tube baby treatment and infertility treatment in Indore at affordable price. Backed up by a team of highly skilled doctors and embryologists, we employ latest fertility techniques in our state of art laboratory, making us one of the Best IVF centers in MP. If you are looking for the best centre for IVF in Indore if yes, contact to Mohak Infertility Centre. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com
OBJECTIVE: The aim of this study was to explore the benefits of in vitro fertilization (IVF) for patients and hospitals under different protocols and if IVF treatment should be incorporated into health care.
PERSPECTIVE: The government should consider including IVF treatment in health insurance. Hospitals and patients could obtain the best benefit by following the hospital’s recommended protocol.
SETTING: This retrospective study was conducted from January 2014 to August 2017 at an academic hospital.
METHODS: A total of 7440 patients used gonadotropin-releasing hormone agonists (GnRHa) protocol, 2619 patients used, gonadotropin-releasing hormone antagonists (GnRHant) protocol, and 1514 patients used GnRHa ultra-long protocol. Primary outcomes were live birth rate (LBR), cost-effectiveness, hospital revenue, and government investment.
RESULTS:
The cycle times for the GnRHa protocol and the GnRHa ultra-long protocol were significantly higher than the GnRHant protocol. Patients who were ≤29 years chose the GnRHant protocol. The cost of a successful cycle was 67,579.39 ± 9,917.55 ¥ and LBR was 29.25%. Patients who were >30 years had the GnRHa protocol as the dominant strategy, as it was more effective at lower costs and higher LBR. When patients were >30 to ≤34 years, the cost of a successful cycle was 66,556.7 ± 8,448.08 ¥ and the LBR was 31.05%. When patients were >35 years, the cost of a successful cycle was 83,297.92 ± 10,918.05 ¥ and the LBR was 25.07%. The government reimbursement for a cycle ranged between 11,372.12 ± 2,147.71 ¥ and 12,753.67 ± 1,905.02 ¥.
CONCLUSIONS: The government should consider including IVF treatment in health insurance. Hospitals recommend the GnRHant protocol for patients <29 years old and the GnRHa protocol for patients >30 years old, to obtain the best benefits. Patients could obtain the best benefit by using the protocol recommended by the hospital.
It is not an easy thing to understand the plight of childless, married couples but we at Mohak Infertility Centre try to do so by offering the best of Infertility Treatment Packages. Mohak Infertility Centre is a one of the Best infertility hospitals in Indore, India. We provide the best IVF, IUI, ICSI, test tube baby treatment and Infertility treatment in Indore at affordable price. If you are search for the Best IVF center in MP come at Mohak Infertility Centre. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com
Gender differences in the adjustment to infertility have been widely discussed in the literature, namely focusing on differences between men and women regarding psychological symptoms and emotional responses and on differences attributed to parenthood. Findings document that in general women reported higher emotional difficulties than men in almost every stages of infertility (Holter, Anderheim, Bergh, & Moller, 2006; Markestad et al., 1998), although patterns of reactions along the infertility experience are similar (Boivin et al., 1998). When examining gender differences on the importance attributed to parenthood, no differences have been found (Moura‐Ramos, Gameiro, Canavarro, Soares, & Santos, 2012). As a result, it has been argued that gender differences on the adjustment to parenthood may be due not to different experiences of infertility and ART, but due to differences in expressing and reporting emotional difficulties (Edelmann & Connolly, 2000). However, we should also consider that unintended childlessness may have a different meaning for men and women (Berg, Wilson, & Weingartner, 1991) and therefore a different impact on their adjustment to infertility and assisted reproduction. Consequently, it may be that the processes by which their distress is affected are different.
The present study
In this study, we investigated the association between infertility history (i.e., duration of infertility and number of previous ART treatment cycles) and emotional adjustment in couples undergoing ART. More specifically, this study investigated the indirect effect of infertility history on emotional adjustment through influencing representations of the importance of parenthood and childlessness, while accounting for gender differences in those effects. We aim to clarify some inconsistencies observed in the literature regarding the role of infertility history on the emotional adjustment of infertile couples. Understanding how patients’ infertility history relates to their emotional adjustment during ART treatment will contribute to a more comprehensive view of the adjustment process to infertility. This understanding may help fertility health care services to identify patients who are at higher risk for emotional distress and stages at which patients may need more support and to delineate targeted interventions to the patients.
Indirect effects of history of infertility on men and women’s emotional adjustment
The results of the present study underline that adjustment to infertility is a highly personal experience, influenced by previous experience and by each person’s own representations of the importance of parenthood in their own lives. Indeed, duration of infertility and number of past ART treatments only affected adjustment indirectly, by affecting men and women’s representations of parenthood.
Young worried couple paying to experienced doctor for visit
The number of previous ART treatments influenced men’s adjustment but not their partner’s. Men in couples who had undergone a greater number of treatment cycles attributed a lower importance to parenthood and had fewer symptoms of depression and anxiety. A higher number of previous treatments, as suggested by Boivin et al. (1995), may have confronted patients with the increasingly more probable prospect of childlessness, promoting its acceptance and reducing their distress, which is underlined by the indirect effect found in the study. At the time the sample was recruited, ART in public settings in Portugal was limited to three cycles, unless otherwise clinically recommended. Men undergoing more treatment cycles could have adjusted their expectations to more easily accept future childlessness. These men may have perceived themselves as having diminished options to achieve parenthood, due to financial (having to move to private clinics) or medical reasons (lower chances of conceiving after three cycles, Pinborg, Hougaard, Andersen, Molbo, and Schmidt, 2009), resulting in less emotional difficulties. According to Lazarus and Folkman (1984), the persistence of a chronic stressor (such as repeated failures in pursuing treatment to achieve pregnancy) can give the opportunity to address its demands, by developing new goals and replacing or reappraising old ones. However, this response pattern was not found for women. The number of previous ART cycles did not affect women’s emotional adjustment directly or indirectly, and it was not associated with representations regarding the importance of parenthood in one’s life. This result was surprising, as it would be expected that past treatment failure would be associated with emotional adjustment (Boivin et al., 1995).
According to this argument, it could also be considered that longer infertility would be associated with lower distress; however, this did not occur. The pattern of association between duration of infertility and couples’ emotional distress was clearly distinct, as this association was positive and curvilinear, apart from the effect on women’s depression. Men with longer infertility reported higher importance for parenthood, which was associated with their anxiety and depressive symptoms. Duration of infertility was not associated with the number of previous ART treatment cycles; therefore, we can presume that some couples had periods of time during which their infertility was untreated and unresolved. This may have increased their emotional difficulties by sustaining expectations regarding treatment and by not allowing for the confrontation of treatment failure. Conversely, depression tended to be lower in women with longer infertility, namely those trying to get pregnant for more than 6 years. Considering that couples in our study were entering treatment, which is a moment of high uncertainty and hope, it can be expected that anxiety is heightened but feelings of loss, which are related depression, may be decreasing after a long‐time experiencing infertility. Nevertheless, this result was surprising and future studies should clarify this issue.
In summary, these results suggest that the resolution and acceptance of the infertility condition occurs not after a long duration of infertility but as a consequence of the experience of repeated ART treatment failure. It seems that it is the process of dealing with treatment failure, confronting couples with childlessness, leads couples to reappraise their life goals and expectations for the future. Couples, who have difficulty envisioning themselves in the future without children and believe that parenthood is the major goal of their life, tend to experience psychological distress when entering treatment. Previous research has shown that this distress is accentuated if they experience failure (Verhaak, Smeenk, Evers et al., 2005; Verhaak, Smeenk, van Minnen, Kremer, & Kraaimaat, 2005). Early detection of these difficulties can be important for professionals to help couples dealing with this distress.
Gender differences on the effects of history of infertility on emotional adjustment
This study showed that the number of previous ART cycles and the duration of infertility affected women’s and men’s adjustment differently. Having undergone a higher number of treatment cycles may have confronted men with the increasingly more probable prospect of childlessness, promoting its acceptance and reducing their distress, but it did not occur with women, who probably envision every new ART cycle as a moment of hope for achieving pregnancy. This is coherent with past research that underlines that men are more prone to consider treatment termination (Greil, Leitko, & Porter, 1988; Sydsjo, Ekholm, Wadsby, Kjellberg, & Sydsjo, 2005), which may translate in easiness to accept future childlessness when compared to women (Peddie, van Teijlingen, & Bhattacharya, 2005; Volgsten, Skoog Svanberg, & Olsson, 2010). These results should be interpreted considering the specificities of the Portuguese social and cultural context, which shapes gender roles and expectations regarding parenthood. Indeed, as other southern European countries, Portugal has rooted traditional views on family and gender roles (Nishioka, 2003) and is conservative regarding parenthood and children. Indeed, although children are equally important for men and women (Aboim, 2007), they play a core role in women’s identity making more difficult for them to accept future childlessness.
Examining the effect of duration of infertility in men’s and women’s adjustment also underlines how the processes of adjusting can be different among couple partners. While it is clear that being unsuccessfully trying to get pregnant is associated with an increase in psychological symptoms, with a tendency to accentuate in the later years, women’s depressive symptoms are an exception. To interpret these results, we should bear in mind that data were collected in the beginning of treatment, which is a moment of heightened hope and expectations (Benyamini, 2003). In this situation, women who have been infertile for a long time but are now in treatment may exacerbate positive emotions (hope, optimism) and diminishing depressive symptoms. In men, the process was the opposite, which may be the result of a lower involvement with the treatment procedures, preventing the experiencing of positive emotions that occur in the beginning of the treatment after several years infertile, associated with a lower use of positive reframing in that situation in order to better adapt to it (Jordan & Revenson, 1999). These results underline how different may be the experience of undergoing assisted reproduction treatments and that couple members may cope differently with past experiences. Nevertheless, more studies are needed to further explore the different mechanisms affecting men and women’s adjustment to infertility.
Strengths and limitations
A major contribution of the present study was the test of nonlinear and indirect associations contributing to the effect of infertility history on emotional adjustment in couples entering ART. Albeit several studies have previously examined the influence of clinical variables on couples’ adjustment, these results contributed to highlight the process by which that influence operates. The inclusion of both couple members within a dyadic design that explores the experiences of both men and women while controlling for the non‐independence of couples’ scores (Kenny et al., 2006) was an important contribution, as it allows studying the specificities of adjustment in men and women while controlling for the interdependence of their experience.
The identification of infertility history as a significant predictor of emotional adjustment is an important contribution because it allows health care providers to direct their attention to more specific characteristics of infertile couples presenting for ART and to target their interventions in order to meet the specific needs of each couple. Additionally, it highlights the importance of referral of infertile patients to fertility clinics in due time.
In addition to the aforementioned contributions, several limitations of the present study are worth noting. The sample size is small, which reduces the power to detect a significant effect; therefore, small effects could have been detected if the sample was larger. The cross‐sectional design does not allow the establishment of causality. Future studies should focus on investigating the impact of infertility history in couples’ long‐term adjustment and in different stages of ART treatment. Lastly, when interpreting these results, it is important to take into consideration the regulation constraints of ART in Portugal, as the law regulating assisted reproduction was developed in 2006 and fully applied since 2009. Therefore, when participants from this study started to try to get pregnant, the referral routine was not well established, and the timely referral for the fertility care would largely depend on the geographical zone of residence of the patients and on each medical centre approach.
Implications for research and clinical practice
The results of our study have several implications for research and for clinical practice with infertile couples. First, studies directed at further investigating the impact of infertility history on adjustment should consider the nonlinearity of the associations between these variables. It is noteworthy that some of the linear or direct associations that were tested were non‐significant, which would have led us to conclude that history of infertility did not have any impact on the couples’ adjustment. It is then important to explore more complex patterns of associations. Second, our results highlight individual variability in the experience of infertility and ART treatments, which was related to the past experience on infertility and to the different meanings attributed to parenthood and childlessness. Indeed, although recognized as a stressful life event for all couples, undergoing ART treatments may impose distinct demands on couples depending on their previous infertility history. Therefore, patients at different treatment phases may require different types and levels of support. Additionally, results underline the role of sociocultural differences that may shape the importance attributed to parenthood. Therefore, these results can be translated in recommendations for health care, namely (1) to develop health policies to ensure that couples who meet the criteria for infertility diagnosis are directed to infertility centres in a timely manner; (2) that psychosocial interventions directed at couples who present emotional difficulties when entering an ART programme consider their previous infertility history and discuss all treatment scenario possibilities and consequences; (3) to discuss the meaning of parenthood and childlessness with couples, to adjust their expectations regarding treatment; and (4) to assure that fertility care takes into account cultural, social, and religious differences that are known to affect the importance attributed of parenthood and therefore the adjustment to infertility.
Mohak Infertility Centre is one of the Best IVF center in Indore. Mohak Infertility Centre offers a complete range of Assisted Reproductive Technology (ART) services, all under one roof. we ensuring that our patients do not have to travel to multiple locations for all their required services. We offer all type of Male, Female Infertility Treatements like IVF, IUI, ICSI, test tube baby, Egg donation and infertility treatment in Indore. Our center is led by the acclaimed Dr Shilpa Bhandari one of the best IVF specialist in Indore with over 10 years of experience, supported by a team of dedicated expert consultants, nurses, healthcare assistants, and embryologists. If you are looking for the Best fertility hospital in India come to Mohak Infertility Centre at Indore, MP. Book an appointment Today Call now 78980-47572 / 80852-77666 For more information, visit – https://www.mohakivf.com
Premature Ovarian Failure also called primary ovarian insufficiency, this disorder is usually caused by an autoimmune response or by premature loss of eggs from your ovary (possibly from genetics or chemotherapy). The ovary no longer produces eggs, and it lowers estrogen production in women under the age of 40.
Call 78980–47572 / 80852–77666 to get the answer of all your queries related to infertility from the best fertility specialist or For more detail
visit our center : SAIMS Campus,Indore-Ujjain state highway,Near MR-10 crossing,Indore (M.P.)-453111
IVF centre in india, Best infertility hospital in indore, ivf specialist in indore, ivf center in indore, test tube baby center in indore, ivf treatment cost in indore, Best centre for IVF in indore, affordable ivf cost in indore, best fertility hospital in india, best ivf center in mp, infertility treatment in indore, best, ICSI treatment in indore
No more wait for #GoodNews , choose #IVF, Choose Mohak.
Call 78980–47572 / 80852–77666 to get the answer of all your queries related to infertility from the best fertility specialist or For more detail
No more wait for #GoodNews , choose #IVF, Choose Mohak.
Call 78980–47572 / 80852–77666 to get the answer of all your queries related to infertility from the best fertility specialist or For more detail https://www.mohakivf.com/
visit our center : SAIMS Campus,Indore-Ujjain state highway,Near MR-10 crossing,Indore (M.P.)-453111
visit our center : SAIMS Campus,Indore-Ujjain state highway,Near MR-10 crossing,Indore (M.P.)-453111
Best infertility hospital in indore, ivf specialist in indore, ivf center in indore, test tube baby center in indore, ivf treatment cost in indore, Best centre for IVF in indore, affordable ivf cost in indore, best fertility hospital in india, best ivf center in mp, infertility treatment in indore, best ivf centre in india, ICSI treatment in indore
Best infertility hospital in indore, ivf specialist in indore, ivf center in indore, test tube baby center in indore, ivf treatment cost in indore, Best centre for IVF in indore, affordable ivf cost in indore, best fertility hospital in india, best ivf center in mp, infertility treatment in indore, best ivf centre in india, ICSI treatment in indore