Best Infertility Hospital in Indore : –Mohak infertility center is a part of a multispecialty advanced care facility located in the heart of India – Indore. Our center was established in 2010 as a part of an effort to provide much need quality infertility care at an affordable cost. Mohak Laparoscopy Hospitals and infertility center is one of the most highly respected and well-established fertility clinics in India, with a patient population that is local, national and international. The physicians and the professional staff of Mohak Laparoscopy Hospitals and infertility center are proud to offer IVF, andrology, embryology, assisted reproductive technology and IVF financing at our fertility center.
Mohak IVF Center, one of the Best Infertility Hospitals in Indore, india provides you International Standard Infertility Treatment along with assisted reproductive technologies like IUI, IVF, ICSI ,etc at affordable IVF treatment cost / Test tube Baby Treatment along with the satisfaction of being consulted by the most renowned IVF specialist in Indore ,M.P. Come join best centre for IVF treatment in indore in our voyage towards better healthcare facilities for infertile couples and experience the Best Infertility Treatment in Indore.
IVF Specialist in Indore : – Dr Shilpa Bhandari is one of the first reproductive medicine specialist of this country. She has not only been a pioneering force in the development of an MCI recognized DM/ McH reproductive medicine curriculum, but has also procured this prestigious super specialization by 3 years of extensive training in this field.
Dr Shilpa Bhandari has always been a meritorious student. She was first in the entire state of Madhya Pradesh in her 12th examinations. She got selected in her favored field of medicine in the first go and pursued her MBBS education through scholarship. In her first year MBBS itself, she was awarded 1 lakh rupees scholarship for securing maximum marks as well as distinction in all subjects. Throughout her 5 years of MBBS she excelled in her studies and secured gold medals in almost all subjects.
From the very beginning Gynaecology fascinated her and she got through all entrance examinations in her first attempt. She opted to study gynecology in the government medical school in Bhopal. Here she underwent gruelling training in all aspects of patient care, surgeries and research.
She has been in active clinical practice since 2007 wherein she has been doing all types of laparoscopic surgeries, managing patients and planning their therapies. Dr Shilpa Bhandari was awarded the opportunity to enhance her skills in the field of reproductive medicine via a 3 year super-specialization. This tenure provided her with the opportunity to hone her focus to the very specific area of infertility and refine her skills in all aspects related to it. In last 8 years she has single handedly established and successfully run the department of reproductive medicine.
She looks after the needs of more than a thousand patients annually in terms of consultation, surgeries, IVF, medical treatment, etc. she has also been actively involved in training other doctors as well as research. She has authored more than 20 research papers in national and international journals. Dr Shilpa Bhandari is an ardent believer in open patient communication, maintaining and honest doctor patient relationship and patient empowerment. Her dream is to provide affordable, honest patient care to couple seeking to enhance their families.
Best IVF centre in India :- Mohak Infertility Centre is a India’s leading Best IVF centre in Indore, India which providing ICSI Treatment in Indore at reasonable cost with best way to improve results.
Infertility Treatment in Indore : – Mohak Infertility Centre is one of the infertility treatment hospital in indore who provides high success rate infertility treatment in indore at affordable cost. its famous Best centre for IVF in indore.
Mohak Infertility Centre is one of the best Test tube baby centers in Indore. Providers the Best infertility treatment at Mohak Infertility Centre Indore. Our doctor is well experienced in IVF treatment and have many client which are satisfied with their treatment. If you are looking the Best centre for IVF in Indore? Mohak Infertility Centre is a India’s leading IVF center in Indore. You can visit us to find more detail about us or contact us to schedule your appointment with us. Call now 7898047572 For more information, visit – https://www.mohakivf.com
अपनी बाहों में अपने बच्चे को भरना जीवन की सबसे बड़ी खुशियों मे से एक है।
मोहक IVF के साथ सुनिश्चित करें अपनी खुशियाँ ।
आईवीएफ एक फर्टिलिटी उपचार है जिसमें अंडों को शुक्राणु (sperm) से अप्राकृतिक (artificially) तरीके से मिलाया जाता है। यह प्रक्रिया मेडिकल लेब में नियंत्रित परिस्थितियों में की जाती है। यह प्रक्रिया इंफटिल दम्पति, और उन लोगों के लिए सहायक है जिनको कोई जननिक (genetic) दिक्कत या परेशानी है|
निःसंतानता का समाधान आईवीएफ के द्वारा संभव है|
अधिक जानकारी के लिए कॉल करें 78980–47572 / 80852–77666 या — https://www.mohakivf.com व्यक्तिगत परामर्श हेतु विजिट करे श्री अरबिंदो मेडिकल कॉलेज परिसर, इंदौर-उज्जैन, स्टेट हाईवे, सांवेर रोड, इंदौर
Best infertility hospital in indore, ivf specialist in indore, ivf center in indore, test tube baby center in indore, ivf treatment cost in indore, Best centre for IVF in indore, affordable ivf cost in indore, best fertility hospital in india, best ivf center in mp, infertility treatment in indore, best ivf centre in india, ICSI treatment in indore
Mohak laparoscopy and infertility center is a part of a multispecialty advanced care facility located in the heart of India – Indore. Our center was established in 2010 as a part of an effort to provide much need quality infertility care at an affordable cost. Mohak Laparoscopy Hospitals and infertility center is one of the most highly respected and well-established fertility clinics in India, with a patient population that is local, national and international. The physicians and the professional staff of Mohak Laparoscopy Hospitals and infertility center are proud to offer IVF, andrology, embryology, assisted reproductive technology and IVF financing at our fertility center.
Mohak IVF Center, one of the Best Infertility Hospitals in Indore, india provides you International Standard Infertility Treatment along with assisted reproductive technologies like IUI, IVF, ICSI ,etc at affordable IVF treatment / Test tube Baby Treatment cost along with the satisfaction of being consulted by the most renowned IVF specialist in Indore, M.P. Come join best centre for IVF treatment in indore in our voyage towards better healthcare facilities for infertile couples and experience the Best Infertility Treatment in Indore.
What makes us special?
Expertise
Fertility professionals are physicians who have pursued additional education for the medical or surgical remedy for infertility. Fertility experts dedicate all or a completely massive percent of their exercise to treating infertility. Our center boasts to have one of the first reproductive medical specialists of India as a full time consultant. Dr Shilpa Bhandari has done her super specialization (DM) in reproductive medicine and oversees the entire treatment cycle of each patient who walks into the clinic.
The team of care providers at Mohak is qualified, dedicated personnel who have worked with us since the day of inception. This makes the center unique because to most of us this is a home and we extend the same level of comfort and warmth to all our patients.
Similarly, due to the fact your treatment is based on your physiological needs, not a workplace timetable, our fertility specialists and a group of workers are available seven days every week and are committed to the time- and exertions-intensive nature of the fertility treatment regimen. This form of dedication is a necessity for the correct guide of your desires and the finest warranty of a successful outcome.
Excellence in care
Infertility management is a long and arduous path. There are many ups and down many failures and successes. It has been our privilege to deliver more success stories and good news to our patients that most centers. We strive to ensure that everyone who walks in our center goes home with a smile on face and a baby in arms. We are very proud of the thousands of successes Mohak Laparoscopy Hospitals and infertility center has celebrated with our patients over the years.Thanks to our team ,our state-of-the-art technology, our world-class ART labs, and our patient-centered approach, it has been our privilege to help all of these families achieve their cherished dream of bringing home a baby.
Empathy
Each person who works in the clinic has been specially trained to understand infertility not only from the point of view of a medical personnel, but also from the point of a patient so we provide you with utmost professional care with a personal touch. We understand what a patient goes through when trying to start a family. Here at Mohak you don’t have to rush through to make way for the next person. This center provides you an opportunity to describe, discuss and understand the treatment.
At Mohak Laparoscopy Hospitals and infertility center, our commitment to seeing every patient as a unique individual is central to our success. You are not a statistic. From the very beginning of each diagnostic consultation, we will work closely with you to create an individual treatment plan designed to give you your best chance of success.
Experience
One of the most important things in medical practice is to anticipate when things can go wrong and this comes from experience. As most of the team has experience of working together in the field of infertility for more than 10 years, we can make sure that you receive the utmost care that you deserve.
Equipments
Infertility management is a technology-based solution. We have one of the finest classes A IVF lab. No expenses are spared when it comes to maintaining air quality, which in turn reflects on the outcome of our IVF cycles. We have the best of equipments which are maintained and upgraded regularly to ensure that the treatments provided are always at par with international standards.
Evidence Based Treatments
A man without data is just a man with a voice. Here when we initiate any treatment, it is always an after and expertise dialogue with the couple and with adequate logic and evidence from research from all over the world. Therefore, during your treatment as a patient not only will you be actively involved in the same, but will also know at all times what is going on and why?
Economical
Our center was established by doctors who started their practice in the one of the poor areas of Indore. Having catered to patients from lower socio economical for more than 30 years. We understand the financial implications of infertility treatments and the strain that it puts onto the pockets of patients. Therefore, it has been our sincere endeavor to provide the most economically effective care for our patients without considering our personal profits.
Ergonomical
Do you want to move to 10 different locations for 1 treatment? No one does. Therefore, we provide one-stop solutions for all your infertility related problems. From laparoscopy to sonography, from blood tests to IVF – we will take care of your needs all the time at one place only.
Evaluation
Despite the best of effort sometimes patients don’t get what they deserve in terms of result. We at Mohak have had the honor to take care of patients who have had multiple failed in the past and we still have been able to give them good results. We take extra time to look for small reasons of failure and improves on them. Though few, we go an extra mile for patients who did not conceive with us in their first attempt and provide concessional therapy for their next cycle.
Infertility is one of the biggest concern in today’s world in both men and women it takes a toll on the dreams of parenthood. With the modern lifestyle that people, posses these days, infertility has turned out to be a common ailment. The advancements of modern technology have made it possible to indulge in a wide range of solutions from the best fertility care provider. If you are search gor the Best centre for IVF in Indore? Mohak Infertility Centre is one of the leading Best infertility hospital and Test tube baby centers in Indore, India and is known for its high success rate treatments in the field of fertility care. We provide treatments like IVF treatment, IUI treatment, ICSI, sperm and egg donation. If you are trying to get pregnant for a very long time but you have had no success in it, then consult with experts at our fertility center, they will surely provide you with the necessary solution to get conceive. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com
WELCOME TO MOHAK LAPAROSCOPY HOSPITAL AND INFERTILITY CENTRE
Dr Shilpa Bhandari is one of the first reproductive medicine specialist of this country. She has not only been a pioneering force in the development of an MCI recognized DM/ McH reproductive medicine curriculum, but has also procured this prestigious super specialization by 3 years of extensive training in this field.
Dr Shilpa Bhandari has always been a meritorious student. She was first in the entire state of Madhya Pradesh in her 12th examinations. She got selected in her favored field of medicine in the first go and pursued her MBBS education through scholarship. In her first year MBBS itself, she was awarded 1 lakh rupees scholarship for securing maximum marks as well as distinction in all subjects. Throughout her 5 years of MBBS she excelled in her studies and secured gold medals in almost all subjects.
From the very beginning Gynaecology fascinated her and she got through all entrance examinations in her first attempt. She opted to study gynecology in the government medical school in Bhopal. Here she underwent gruelling training in all aspects of patient care, surgeries and research.
She has been in active clinical practice since 2007 wherein she has been doing all types of laparoscopic surgeries, managing patients and planning their therapies. Dr Shilpa Bhandari was awarded the opportunity to enhance her skills in the field of reproductive medicine via a 3 year super-specialization. This tenure provided her with the opportunity to hone her focus to the very specific area of infertility and refine her skills in all aspects related to it. In last 8 years she has single handedly established and successfully run the department of reproductive medicine.
She looks after the needs of more than a thousand patients annually in terms of consultation, surgeries, IVF, medical treatment, etc. she has also been actively involved in training other doctors as well as research. She has authored more than 20 research papers in national and international journals. Dr Shilpa Bhandari is an ardent believer in open patient communication, maintaining and honest doctor patient relationship and patient empowerment. Her dream is to provide affordable, honest patient care to couple seeking to enhance their families.
If you are looking for the Best infertility treatment hospital with Best IVF specialist in Indore Mohak Infertility Centre is india’s leading Infertility treatment hospital and IVF center in Indore. Childlessness can be the most agonizing feeling for parents. To facilitate infertility-ridden couples with the boon of a child, Dr. Shilpa Bhandari’s Mohak Infertility Centre has been creating miracles for the past 10 years. It has been recognized as one of the Best IVF centers in MP. mohak infertility centre offers the most advanced fertility treatment by utilizing modern medical technologies, state of the art infrastructure and personalized care. Dr. Shilpa Bhandari is one of the finest IVF specialists in our country who has produced numerous successful results in extreme cases. Hence, if infertility problem has kept you waiting long enough, it is the right time to consult our IVF hospital. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com
प्रत्येक दंपत्ति का सपना मां-बाप बनना होता है इसलिए जब वे मां-बाप नहीं बन पाते हैं, तो वे संतान सुख प्राप्त करने के लिए हर मुमकिन कोशिश करते हैं। लेकिन, दुर्भाग्यवश जब किसी भी कारण से वे मां-बाप नहीं बन पाते हैं, तो फिर किसी बेहतर माध्यम की तलाश करते हैं, जिनके द्वारा वे मां-बाप बन सकें।
मेडिकल साइन्स की तरक्की से आज कई ऐसे तरीकें उपलब्ध हैं जिनसे आप मां-बाप बनने का सुख उठा सकते हैं। इन विट्रो फर्टिलाइजेशन या आईवीएफ उन एक तरीकों में से एक है।
निःसंतानता का समाधान आईवीएफ के द्वारा संभव है|
अधिक जानकारी के लिए कॉल करें 78980–47572 / 80852–77666 या व्यक्तिगत परामर्श हेतु विजिट करे श्री अरबिंदो मेडिकल कॉलेज परिसर, इंदौर-उज्जैन, स्टेट हाईवे, सांवेर रोड, इंदौर
Children’s are God’s Best Creations… They spread happiness and joy in every season.Handle them with love and care. Happy Children’s Day
At Mohak Infertility Center– An Infertility Treatment Hospital in Indore that brings a hope to childless couples, provides IVF, IUI, ICS, Male & Female, Test tube baby treatment and Infertility treatment in Indore One of the Best IVF centre in Indore.
To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
During unexplained infertility, you CAN CONCEIVE NATURALLY after an IVF treatment. In such cases, pregnancy can also be totally normal. The factors affecting natural conceptions can be stress or age.
To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
Transvaginal hydrolaparoscopy is a culdoscopic approach for the inspection of the posterior pelvis, but, in contrast to culdoscopy, uses an aqueous solution for the distension of the pelvic cavity and small diameter optics. The technique is used for diagnostic purposes in patients with infertility and is performed under local anesthesia or conscious sedation in an ambulatory surgical center. We report on a continuous series of 1,000 patients with infertility and without obvious pelvic pathology. Access and good visualization was obtained in 96.8% of the patients. The main complications were intraperitoneal bleeding and bowel perforation, which after the initial period occurred respectively in 1.9 and 0.1%. All complications were managed conservatively, and no major complication occurred. Clinically significant pathology was diagnosed in 25% of the patients, which allowed immediate triage of the patients for further management. Transvaginal hydrolaparoscopy can be proposed as a first line technique to replace hysterosalpingography and diagnostic laparoscopy in the exploration of patients with unexplained infertility.
Introduction
In Europe over the past 40 years, endoscopic evaluation of the pelvis has become an integral part of the infertility work-up. In routine practice, hysterosalpingography (HSG) is the first-line investigation and, if normal, laparoscopy is frequently delayed for 6 months or more. Laparoscopy is indeed an invasive procedure, associated with potentially serious complications, and together with hospitalization it can also be an expensive procedure. On the other hand, HSG is inferior to the chromopertubation test for the diagnosis of tubal patency [1] and also has a low sensitivity for the diagnosis of pelvic endometriosis and adhesions. If laparoscopy is performed as a first-line investigation on all infertile patients, there will be a large number of patients with normal findings or with minor pathology that has no or doubtful impact on the management of infertility.
It has been argued that with the advent of ART, laparoscopy can be omitted from the infertility work-up when there is no abnormal contributing history and the HSG is normal and, as a consequence, the cost of fertility treatment is reduced without compromising success rates [2]. Karande et al. [3], however, found in a prospective randomized trial that a higher pregnancy rate with lower costs is achieved with a traditional treatment algorithm than with IVF-embryo transfer as a first line-therapy.
We therefore wish to report on a continuous personal (H.V.) series of 1,000 procedures of transvaginal laparoscopy (THL), which were performed in combination with the mini-hysteroscopy and chromopertubation test as a first-line investigation of female infertility [4]. The combination of the three procedures has been coined transvaginal endoscopy (TVE).
Materials and methods
THL was discussed with all women who met prospectively established exclusion and inclusion criteria. In all patients, the indication was primary or secondary infertility. The patients had a complete history, physical examination and transvaginal sonography. Patients were excluded if they had an indication for operative laparoscopy, abnormal pelvic findings such as fixed retroverted uterus, rectovaginal endometriosis, large ovarian cyst or obliterated cul-de-sac, or an upper vaginal stenosis. Patients with vaginal or pelvic infection were first treated before THL was performed.
THL was used as described by Gordts et al. [5]. With the patient in the dorsal decubitus position, only a limited amount of fluid is required to have the tubo-ovarian structures floating in the excavation of the posterior pelvis. We used a narrow-diameter (<3.5 mm), foroblique 30°, wide-angled and rigid optic, a high intensity light source and a digital camera. Inspection of the pelvic structures was achieved without grasping or manipulation. At the end of the procedure a chromopertubation test was performed and, when indicated, salpingoscopy was added. All interventions were performed under conscious sedation as an office procedure in an outpatient surgical suite.
Transvaginal laparoscopy was considered complete if the tubo-ovarian structures, pelvic sidewalls and cul-de-sac could be seen, or if pathology was diagnosed that indicated the need for operative intervention or ART.
Results
A total of 1,000 THLs were performed during the period starting from 1998 until 2003. Thirty-two (3.2%) failures occurred with failed access in 11 (1.1%) and absent or poor visualization in 21 (2.1%). In total, 968 (96.8%) of the procedures were completed. No pathology or pathology of minor clinical significance was found in 736 (76%). In the group with completed procedures, unexpected clinically significant pathology was diagnosed in 240 (25%) and included mainly ovarian endometriosis, tubo-ovarian adhesions, isthmic block and hydrosalpinges. The diagnostic findings resulted in 36 (3.7%) operative laparoscopies and 204 (21.1%) medical therapies and ARTs.
No major complication occurred in this series. Intraperitoneal bleeding was seen in 23 (2.3%) of the patients and occurred on the posterior wall of the uterus (n=13), parametrium (n=2), ovary (n=2), omentum (n=1) and adhesions (n=5). Bowel perforation occurred in 5 (0.5%) and was managed conservatively with antibiotics. Infection occurred in two (0.2%).
The correlation of the failures (no access or no visualization) with the experience showed that 5 (10%) failures occurred in the first 50 procedures and 26 (2.8%) in the subsequent 950 procedures (P=0.018). Bleeding occurred in 5 (10%) of the first 50 cases and 18 (1.9%) of the following 950 cases (P=0.004). Bowel perforation occurred in 4 (8%) of the first 50 cases and in 1 (0.1%) of the following 950 cases (P<0.0001).
Discussion
By using TVE as a first-line investigation of female infertility, we avoided HSG in 96.8% and laparoscopy in 93.2% of the patients. In 24% of the patients, unexpected major pathology was diagnosed and recommendations for operative laparoscopy, medical therapy or ART could be made.
Several studies have validated the feasibility, reproducibility, diagnostic accuracy, acceptability and safety of the procedure [6]. Different centres have reported access in over 95% and normal findings in 41 to 59% of the cases. In this series of 1,000 consecutive cases, access and visualization of the pelvic structures were achieved in 96.8% of the patients. The performance of THL is defined by visualization of the ovaries, fallopian tubes, posterior wall of the uterus, ovarian and uterosacral ligaments, sidewall of the posterior pelvis and cul-de-sac. In this series, these structures were normal or showed pathology of minor significance in 76% of the patients.
The potentially serious complication of transvaginal access is rectal perforation and sepsis. In a survey of 3,667 procedures the incidence of bowel perforation was 0.65%, which decreased after the initial experience to 0.25%. No delayed diagnosis and sepsis occurred, and 92% of the cases were managed with outpatient antibiotics [7]. In the present series minor bleeding occurred in 2.5% and bowel perforation in 0.5% of the patients. Analysis of the occurrence of complications in function of experience confirmed the importance of the learning curve. After the initial 50 cases, the complication rate of intraperitoneal bleeding and bowel perforation decreased significantly to 1.9 and 0.1%, respectively. It should, however, be noted that even in experienced hands these complications can occur and, therefore, the patients need to be informed. However, in this series no major complication such as sepsis occurred and, similar to previous series, most bowel perforations were managed conservatively with antibiotics without consequences.
As a first-line procedure for the investigation of female infertility, TVE is in direct competition with HSG. The prognostic value of the chromopertubation test has been shown to be better than that of HSG [1]. Four authors reported abnormal findings at THL in 44% of 241 patients with normal or suspected hysterosalpingography [6]. Shibahara et al. [8] compared HSG versus THL in a series of patients with and without a history of Chlamydia infection and found that THL was superior for the diagnosis of peritubal adhesions. The additional advantage of THL for tubal exploration is the ability to examine directly the tubal mucosa by salpingoscopy. Salpingoscopy is a better predictor for pregnancy outcome after tubal reconstructive surgery than routine investigation by HSG and standard laparoscopy [9, 10].
Fatum et al. [2] suggested that in patients with a normal HSG, laparoscopy would be superfluous and patients should undergo up to six cycles of gonadotropins and IUI and then undergo IVF if they continue to be infertile. However, in a recent study Capelo et al. [11] found significant pelvic pathology in one third of the patients failing to conceive after four ovulatory cycles of clomiphene citrate and concluded that early endoscopic diagnosis of such pathology would have allowed the couple to proceed directly to IVF.
Cicinelli et al. [12] found in a randomized controlled trial that THL in combination with mini-hysteroscopy in an outpatient setting was better tolerated by the patients than HSG. Finally, HSG is a diagnostic X-ray procedure that exposes the bladder, ovary and colon to radiation. The organ-specific radiation doses of HSG for the bladder and colon are estimated at 4.67 and 2.82 mGy, respectively. It is now generally accepted that there is no threshold dose below which radiation exposure does not cause cancer, and the attributable risk of diagnostic X-rays is estimated to range from 0.6 to 1.8 of cases of cancers per year [13].
When an accurate infertility exploration can be performed with a minimally invasive procedure and a reliable treatment exists, an early diagnosis followed by the most appropriate, effective treatment can greatly reduce the monthly failures and the sense of frustration for the couple, particularly when age and time are additional unfavorable factors
Our current approach of exploring female fertility after 1 year or more of infertility may paradoxically lead to undertreatment as well as overtreatment.
Recent prospective population-based studies have demonstrated that the time to clinical pregnancy in most women with normal fertility is not more than 6 months [14, 15]. It can therefore be assumed that already after six cycles with fertility-focused intercourse, irrespective of their age, most women with normal fertility have conceived and that the remaining group is largely composed of couples faced with subfertility. Today, when female fertility can be explored accurately with a minimally invasive procedure, such as TVE [4], and a reliable treatment exists for many major disorders, a prolonged waiting period is outdated.
It is concluded that in women with previously normal cycles infertility should be investigated already after a 6-month period of fertility-focused intercourse and that transvaginal endoscopy, which combines minihysteroscopy and transvaginal hydrolaparoscopy, can be proposed as a first-line technique.
fter a 6-month period of fertility-focused intercourse and that transvaginal endoscopy, which combines minihysteroscopy and transvaginal hydrolaparoscopy, can be proposed as a first-line technique.
Child born through IVF is as normal as Concieved naturally. Various studies proved the fact that there is no karyotypic abnormalities including mosaicism in ART Concieved pregnancy than natural. Developmental milestones and birth rate of an IVF born child is totally normal.
To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
To evaluate the spectrum of diagnostic findings in hysterosalpingography (HSG) examinations performed at our institution between 2006–2010 and their prognostic significance for treatment decisions and fertility outcomes.
Methods
Patients were filtered from our PACS. Pathological HSG studies were re-evaluated. Indications for referral, technical success and diagnostic findings were analysed. Pathological findings were correlated with further diagnostic workups, treatments and fertility outcomes.
Results
Of 411 HSG examinations, 226 (55 %) were normal, 94 (23 %) showed minor abnormalities and 5 (1.2 %) were not diagnostic. Eighty-six (21 %) examinations were pathological. Twenty-nine patients underwent subsequent laparoscopy, during which proximal tubal occlusion diagnosed at HSG was ruled out in 9/23 cases. Follow-up information was unavailable for 20 patients. Nineteen of 66 patients with follow-ups after pathological HSG had at least one subsequent successful pregnancy. Forty-one patients had no further treatment and no pregnancies.
Conclusions
The detection rate for pathologies at HSG was low (21 %). There was a high false-positive rate (39 %) for proximal tubal occlusion, most likely because of spasms, demonstrating the importance of delayed imaging after injection of antiperistaltic agents. HSG remains a valuable diagnostic tool. Our results, however, indicate that this technique should be more selectively indicated.
Main Messages
Good acceptance of HSG by the patients. No complications with antibiotic prophylaxis.
Low detection rate (21 % pathological exams) for pathologies in our study.
High false-positive rate for proximal tubal occlusion.
This demonstrates the importance of waiting longer after injection of buscopan.
High pregnancy rate in pathological cases: Indication too broad or even a therapeutic effect of HSG?
Introduction
Approximately 15 % of couples are affected by infertility, which is defined as the inability to conceive after 12 months of regular unprotected sexual intercourse [1]. Common causes of infertility include male factor (45 %), ovulation disorders (37 %) and tubal damage (18 %) [2]. A combination of several factors is found in approximately 20 % of all couples. The etiology of tubal damage can be intrinsic (ascending salpingitis, including salpingitis isthmica nodosa) or extrinsic (peritonitis, endometriosis and pelvic surgery). The most common causes of pelvic inflammatory disease (PID) are Chlamydia trachomatis, Neisseria gonorrhoeae and multibacterial infections [3]. Studies have demonstrated that the severity of tubal damage found in infertile women is directly related to their serum chlamydia antibody IgG titer (CAT) [4].
Uterine cavity abnormalities can be a contributing cause of subfertility in 10 % of women. Abnormal uterine findings are reported in as many as 50 % of women with recurrent implantation failure [5]. These findings include endometrial polyps or fibroids, which are observed as filling defects or uterine wall irregularities using hysterosalpingography (HSG). HSG can also demonstrate intrauterine adhesions and congenital abnormalities [1].
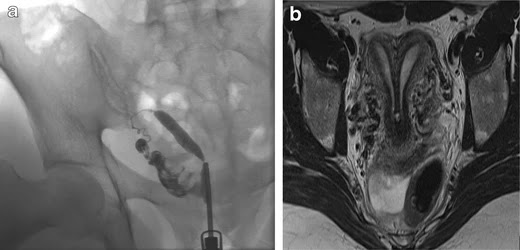
Imaging plays a key role in the diagnostic evaluation of female infertility [6]. Transvaginal ultrasound (TVUS) is a standard, first-choice procedure. Abnormal findings can be further evaluated with saline or contrast hysterosalpingo sonography [1]. Hysterosalpingo contrast sonography (HyCoSy) has been found to be highly sensitive, specific and accurate in identifying uterine abnormalities, e.g., polyps. However, it is of limited value for the assessment of tubal abnormalities. Magnetic resonance imaging (MRI) can be used to evaluate congenital Müllerian duct anomalies and to diagnose adenomyosis, leiomyoma and endometriosis; however, its role in tubal assessment is presently limited [7, 8].
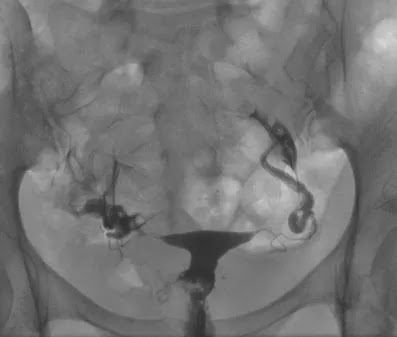
The primary role of HSG is to evaluate the morphology and the patency of the fallopian tubes. The fallopian tubes should appear as thin, smooth lines that widen in the ampullary portion. Tubal abnormalities observed with HSG can be congenital, or due to spasm, occlusion or infection. Tubal occlusion manifests as an abrupt cutoff of contrast material with non-opacification of the distal fallopian tube, and can be unilateral or bilateral. Peritubal adhesions prevent contrast material from spilling into the abdominal cavity and distributing freely [8, 9].
HSG can also be helpful in evaluating uterine cavity abnormalities. It is considered to have a high sensitivity (60–98 %) but low specificity (15–80 %) in detecting uterine abnormalities, and hysteroscopy remains the method of choice for the final assessment. The differential diagnosis of intrauterine filling defects by HSG includes polyps, endometrial hyperplasia, submucosal fibroids, intrauterine adhesions and septa. These findings necessitate further investigation with hysteroscopy to confirm and possibly treat the pathology [1]. In the literature, the results of HSG studies have been shown to be important for selecting patients for diagnostic laparoscopy with chromopertubation [9, 10].
In 2008, guidelines published by the European Society of Human Reproduction and Embryology (ESHRE) recommended that a semen analysis and an ovulation assessment should be performed before a tubal patency test. Women with a high probability of pathological conditions should be offered a first line laparoscopy. This approach has the advantage that any tubal or pelvic pathology can be investigated and treated at the same time. The ovaries can be assessed by TVUS according to the ESHRE guidelines [11, 12]. Following these guidelines, we advise women to undergo a first line laparoscopy combined with hysteroscopy if they have a history of previous pelvic surgery, PID, elevated CAT, or severe dysmenorrhea or dyspareunia.
The purposes of this study were to evaluate all pathologies that were diagnosed by HSG in the workup of female infertility at our institution between 2006 and 2010, to describe the spectrum of diagnostic findings, and to correlate the diagnostic findings with clinical findings and outcomes.
Patients and methods
Patients were identified by searching the radiology information system (RIS) for all HSG examinations from September 2006 (introduction of our Picture Archiving and Communication System; PACS) to April 2010. A total of 411 HSG examinations were identified and included in the study. The ages of the patients ranged between 22 and 42 years, and the mean age was 32.6 years.
For most patients, diagnostics and treatment were performed in our department. Some patients were sent to our department only for tubal assessment by their gynaecologists or family doctors. In selected cases, follow-up information concerning pregnancy or pathological findings was therefore not available.
Our department of gynecology specialises in the diagnosis of infertility and its treatment, including in vitro fertilisation (IVF). The Department of Gynecology as well as the Institute of Radiology are certified by DIN EN ISO 9001:2000. Approximately 450 intrauterine insemination (IUI) cycles and 450 fresh/frozen IVF/intracytoplasmatic sperm injection (ICSI) cycles were performed.
Results
No immediate, i.e., allergy to the iodinated contrast agent or propfol, or delayed, i.e., pelvic infections, complications were observed during or following any of the 411 examinations. Of the 411 HSG examinations, 226 (55 %) were normal. In 15 of the examinations that were assessed as normal, administration of Buscopan® was required to differentiate spastic tubal occlusion from true tubal occlusion. There were minor abnormalities observed in 94 examinations (23 %). Five examinations (1.2 %) were not diagnostic (early termination of the exam due to venous filling of the uterine plexus).
In 86 (21 %) of the examinations, at least one pathology was described that was probably or possibly relevant to female infertility (Table 1). The detailed analysis of our study was based on this subpopulation. There was a statistically significant age difference between patients with normal (mean 31.8 years) and pathological (mean 34.1 years) HSG examinations (P-value = 0.0001).
Of these 86 patients, 30 solely uterine pathologies were identified. The most common uterine pathologies were filling defects (n = 15, Figs. 2 and 3) and Müllerian duct anomalies (n = 11), including arcuate uterus, hypoplastic uterus, uterus septus (Fig. 4) and uterus bicornis bicollis (Fig. 5a and b). A few patients (n = 4) had minor abnormalities of the uterine cavity that were described as likely originating from mucosal irregularities (Table 1).
Additionally, 29 laparoscopies (LSC) and 19 hysteroscopies (HSC) were performed on 34 different patients. Three additional pathologies of the uterine cavity (2 small polyps and a single myoma) were identified that were not visible in the HSG. Nine of the 23 one- or two-sided proximal tubal occlusions diagnosed by HSG were normal at laparoscopy, resulting in a false-positive value of 39 %. On the contrary, HSG showed a high negative predictive value (100 %): No additional tube pathologies were identified at LSC if the tube morphology was normal at HSG. In the nine patients mentioned above, LSC (n = 5) and HSC (n = 4) were combined with an intervention (tuboneostomy, myoma resection or one-sided salpingectomy).
A very common procedure following a pathological HSG was insemination because of male subfertility. This procedure was performed as long as one of the fallopian tubes was described as normal and the uterine cavity had no major pathology.
In total, there were 27 pregnancies in 25 of the 86 patients (including 20 patients lost to follow-up, see below) with a pathological condition at HSG. These pregnancies resulted in the birth of 19 healthy children and 8 miscarriages.
Seventeen of the 25 patients only bore a healthy child. These 17 patients had the following HSG results: one-sided tubal occlusion (n = 6), adhesions (n = 4, one of these with uterus arcuatus), filling defects (n = 5), tubal irregularities, possibly postinfectious (n = 1) and sactosalpinx (n = 1).
Two of the 25 women had miscarriages followed by successful pregnancies. Both of these patients showed filling defects, and one patient had additional tube irregularities, which were possibly postinfectious.
Six of the 25 patients had pregnancies that resulted in spontanteous abortions. In these six patients, the HSG showed one-sided tubary occlusion (n = 2), two-sided tubal occlusion (n = 2), adhesions (n = 1) and an arcuate uterus (n = 1).
Results of further diagnostic workupEleven of the 86 patients had no further diagnostic workups. Three of the 86 patients had diagnostic workups following HSG without surgical procedures or further pathologies identified.
Six of the 86 patients that solely had an miscarriage as the outcome showed the following conditions:
Two-sided tubal occlusion, normal LSC and HSC. Pregnancy after insemination (n = 1).
One-sided tubal occlusion confirmed at LSC (n = 2), ½ with endometriosis at HSC.
Two-sided tubal occlusion, fundus myoma at HSC not visible at HSG (n = 1).
Two-sided tubal occlusion, abortion after ovum donation (n = 1). This patient had no LSC because of her relatively high age.
Uterus arcuatus (ovarian insufficiency) (n = 1).
One of the 86 patients had a miscarriage that was followed by a successful pregnancy. In this patient, the HSG showed a cavity abnormality due to adenomyosis/synechiae. The HSC diagnosis showed multiple scars. An additional myoma that was not visible at HSG was resected (Fig. 3).
Four of the 86 patients had resection of a myoma (n = 3) or a polyp (n = 1) prior to becoming pregnant. Three of these HSG examinations identified filling defects, and one was not visible. One of these four patients had a spontaneous abortion prior to a normal birth. The other three patients gave birth to healthy children.
Forty-one of the 86 patients had no further treatment and no pregnancies. Two of these patients had no wish for further children; the examination was performed to assess the need for anticonception.
For 20 of the 86 (23 %) patients, follow-up information was unavailable. Approximately half of these patients were referred from outside institutions for HSG examinations only, and the remainder were drop-outs from the fertility program.
In our fertility center, HSG is still the most common first-line diagnostic test to evaluate the uterine cavity and tubal patency. HSG is relatively easy to perform and can be completed as an outpatient procedure. Using a good anesthetic protocol with propofol sedation, the procedure is well tolerated by patients. Whereas the administration of Propofol obviously increases patient comfort, the procedure is performed without any sedation in many other institutions, and the advantages should be discussed in light of the additional costs.
As recommended by the ESHRE guidelines [11], we excluded other infertility causes, such as male or ovarian factors, before performing a tubal patency test. According to the ESHRE guidelines, a first-line laparoscopy/hysteroscopy should be performed when tubal, uterine or pelvic pathologies are suspected or detected by TVUS.
In recent years, CAT has become an important screening test that can be used to decide upon further examinations [10]. Hysterosalpingo contrast sonography (HyCoSy) has become an important tool for the diagnosis of uterine or tubal pathologies [12]. According to the literature, this technique has a higher sensitivity than HSG (0.80 versus 0.53) [13], and the specificity (0.84 versus 0.87) is similar for both exams [14].
In our opinion, HyCoSy is more demanding for the examiner than HSG, it is better for assessing the uterine cavity than the fallopian tubes , and it has a longer learning curve. The advantages of hysterosalpingo contrast sonography are that it costs less and causes less pain; therefore, no anesthesia is necessary. Additionally, there is no exposure to radiation.
Whereas HyCoSy and HSG only have diagnostic value, laparoscopy and hysteroscopy also have therapeutic options, including adhesiolysis, excision of endometriotic lesions or resection of intrauterine polyps.
Considering that HSG is far more expensive and invasive (i.e., anesthesia, exposure to radiation) than HyCoSy, our aim is to avoid unnecessary HSG exams. Since 2009, we have routinely used CAT screening to select patients for laparoscopy/hysteroscopy as the first-line exam, and we have set an age limit of 38 years, above which we perform HyCoSy instead of HSG.
During the years of our retrospective study from 2006 to 2010, we chose the diagnostic procedure according to the criteria shown in Table 2. One of the aims of our retrospective study was to improve our decision-making and to avoid unnecessary exams. Of the 411 analysed HSGs, 86 (21 %) demonstrated at least one pathology described as potentially relevant for fertility. This is quite a low detection rate, meaning that we performed four of five HSG procedures in vain. This clearly indicates that the indication for HSG at our institution in recent years was too broad. Furthermore, there was a high false-positive rate for proximal tubal occlusion (39 %) and a high pregnancy rate in patients with pathological HSG, i.e., 25/86 of the total patients and 25/66 of the patients with follow-up.
We acknowledge some limitations to our study. First, the retrospective study design might appear to be a limitation of this study; however, all of the images from the examinations had been archived in our PACS, and all pathological cases were re-evaluated. No follow-up information was available for 23 % of the patients with a pathological condition at HSG. It is not known how many of these patients became pregnant. Dropout rates have been reported in the literature to be as high as 50 % before the beginning of therapy. It is likely that patients interrupt their fertility care because of emotional distress and poor prognoses [15]. Furthermore, some follow-ups were not available in our study for patients sent to our center only for tubal assessments by their gynaecologists or family doctors.
Another limitation is that laparoscopic and/or hysteroscopic results were available in only 29 of 411 HSG patients. This means that there was no information about possibly false-negative exams in the patients with normal HSG exams. From the 86 HSG exams with suspected pathologies, 29 patients had laparoscopy/hysteroscopy, and 20 patients were lost to follow-up. Therefore, it is not known how many of these patients became pregnant.
In conclusion, HSG is a safe, low cost and, with the application of propofol sedation, a well-tolerated procedure for tubal assessment, which should be performed at the end of the infertility investigation protocol. The relatively low percentage (21 %) of pathological exams in our population underlines the need for good patient preselection. The high false-positive rate for proximal tubal occlusion (39 %), probably due to tubal spasm, demonstrates the importance of antiperistaltic agents and delayed imaging. Furthermore, we observed a high pregnancy rate (in patients with pathological HSG). Most cases of pregnancy were spontaneous without tubal or uterine surgery. This could mean that the indication for HSG was too broad or that there could even be a therapeutic effect of the HSG procedure, i.e., improved patency of the fallopian tube because of the flushing during the examination [16]. As a result of this data analysis and literature review, the workflow in our own center will be adapted. We will establish hysterosalpingo-contrast sonography (HyCoSy) as a first-line exam for tubal and uterine factors, and improve the patient selection for primary laparoscopy/hysteroscopy using routine screening for CAT.