With IVF treatment there is no need of complete bed rest. Mild to moderate exercises and household works improve your blood circulation and enhance the rate of implantation. Health of fetus as well as mother can be improved by improvising balance between food, exercise and rest, during pregnancy.
To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
The average age at first birth in the United States has been rising steadily over the past decades, from 21.49 in 1968 to 23.72 in 1985 and 25.26 in 2004. As shown in Fig. 1, this increase has been accompanied by remarkable changes in the age distribution of first-time mothers, which has become less skewed with a substantially higher density of first-time mothers older than 25 and an extension of first-time motherhood beyond the age of 40.
Women, however, face a biological time constraint on bearing children because fecundity decreases with age. The introduction of and the subsequent increase in the use of assisted reproductive therapies (ARTs) have helped women in extending their reproductive lives (CDC 2007). ARTs, particularly in-vitro fertilisation (IVF), are very expensive procedures. For example, in 1992, a birth from an IVF procedure cost between 44,000 and 211,942 USD (Neumann et al. 1994). Over time, however, ART patients have faced substantially lower costs due to increased competition (Hamilton and McManus 2012), a reduced number of cycles due to better technology,1 , 2 and most importantly, the availability of insurance in both the United States and in Europe.3 In this paper, we analyse whether easier access to ARTs induces women to delay motherhood and whether, in the long term, it affects women’s completed fertility by the end of their reproductive lives.
The perception that ARTs increase fertility has led the European Parliament to call on member states to insure ‘the right to universal access to infertility treatment’ (Ziebe and Devroey 2008). This movement’s incarnation in the United States has sponsored several attempts at approving the ‘Family Building Act of 2009’, which would extend coverage for infertility treatments, and the enactment by several states of infertility insurance coverage laws, which are referred to as infertility treatment mandates.4 Considering the high cost of infertility treatments (Bitler and Schmidt 2012; Collins 2001), policy interventions that grant insurance coverage for infertility treatments may affect fertility trends and ultimately, population age structures. The mid- to long-term consequences of ARTs are central to the European debate on possible solutions to an ageing population—i.e., can ARTs be part of a package of policies intended to increase fertility rates in Europe? (Grant et al. 2006; Ziebe and Devroey 2008).5
The answer is complex because the short-term effect of an increase in coverage for infertility treatments may be very different from the long-term effect. In the short term, an increase in the aggregate fertility rate is expected due to an increase in fertility amongst the least fertile women (a compositional effect). Typically, these are relatively old women who delayed motherhood and would be unlikely to conceive otherwise (Buckles 2005; Schmidt 2005a, 2007). Moreover, increased access to ARTs increases the frequency of multiple births in the population (Bundorf et al. 2007). These two effects are short-term and non-strategic and may be referred to as ex-post moral hazard. In the long term, however, easier access to infertility treatments and the possibility of extending reproductive life may induce women to further delay motherhood, possibly because of overly optimistic perceptions about the effectiveness of infertility treatments (Lampi 2006; Benyamini 2003). This response by relatively young women, which may be referred to as ex-ante moral hazard, is strategic and would increase the average age at first birth for several years after the policy was implemented.6 Such a response would be consistent, for example, with the delay in marriage due to increased infertility coverage documented in Abramowitz (2014). Therefore, it is possible that an increase in insurance coverage for infertility treatment may have negative effects on total fertility in the mid- to long-term. This paper examines these issues in the United States, where, by 2001, more than 1 % of live births were due to IVF (CDC 2007).
Our objective in this paper is twofold. First, we analyse the impact of an increase in infertility insurance on the timing of first births. Although this question was first explored by Buckles (2005), we believe that our paper contributes in a substantial way to the few existing manuscripts that address this topic by using more adequate data and methodology. Moreover, we go a step further by looking into the long term effects of increasing infertility insurance. Second, we ask whether the increase in infertility insurance affects completed fertility, i.e., fertility by the end of a woman’s reproductive life. This study represents, to the best of our knowledge, the first to address this issue.7 Both objectives are analysed using data from the United States.
To assess whether infertility insurance induces a delay in motherhood, one needs to combine evidence about reduced fertility of young women with information on when women become mothers, i.e., when (if at all) they stop delaying motherhood. This precisely describes the approach we adopt in the first part of this paper; we not only offer similar evidence as Buckles (2005) on the reduced probability that relatively young women in mandated states have children, but we also demonstrate that the average age of first-time mothers continues to increase in the medium to long term after the enactments of infertility mandates.8 Our long-term estimate (10–16 years after the first and the last mandates were passed) ranges from 3 to 5 months. These effects are substantial insofar as they represent between 15.7 and 18.8 % of the total increase in the age of first-time mothers during the period considered for the group of six states that enacted infertility treatment mandates9 and between 24.8 and 34.3 % for the three states with the most generous coverage (Illinois, Massachusetts, and Rhode-Island).10
The ageing of first-time mothers may impact women’s completed fertility in the long term. Hence, our second goal is to determine whether infertility insurance indeed increases women’s completed fertility by the end of their reproductive lives, a question that has not been addressed in the existing literature. In principle, any potential negative effects on fertility induced by a delay of motherhood may eventually be offset by a higher prevalence of multiple births,11 so the impact of infertility insurance on completed fertility is ultimately an empirical question. Overall, our estimates, based on data on the number of biological children from the June CPS, show no statistically significant effect of either the strong or the comprehensive mandates on completed fertility.
In sum, our paper shows that, despite being associated with higher birth rates among relatively older women and with a higher prevalence of multiple births, infertility insurance does not have a statistically significant effect on women’s fertility at the end of their reproductive lives. The reason lies, as we further show, in the fact that infertility insurance mandates also appear to delay motherhood among relatively younger women and, hence, make conception more difficult because fecundity decreases with age.
The rest of the paper is structured as follows: Sect. 2 describes the characteristics of infertility treatment mandates including where and when they were enacted; Sect. 3 describes the data sources used in this paper; Sect. 4 presents our evidence on the delay of motherhood; Sect. 5 presents an analysis of the impact of the mandates on women’s completed fertility; Sect. 6 presents conclusions; Sect. 7 contains figures and tables; and Sect. 8 is the “Appendix”.
Mohak Infertility Center is one of the Best fertility hospital in india Mohak Infertility Center believe everyone has right to become parents whether he/she is not able to conceive naturally and that’s why we have achieved comparatively high pregnancy rate. Our dedicated and whole hearted efforts make this believe real for various infertile couples. We offer all IVF Treatment under one roof like ICSI-IVF India, IUI, Male/Female Infertility, test tube baby treatment and infertility treatment in indore India. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com
IVF per se is not the indication of cesarian delivery. But the rate of cesarian is higher in patients who have gotten pregnant via IVF. The reasons are – higher age of mother – associated complicating factors like obesity, fibroids , diabetes etc – multiple pregnancies – preterm deliveries
At the end of the day route of delivery depends on factors of patient and pregnancy not on how the baby was conceived.
Get the answer of all your queries regarding IVF from our fertility specialist. To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
IVF does not cause twin pregnancies especially if selected single embryo transfer is done. However many centres choose to do multiple embryo transfers increasing the chances of twin or higher order pregnancies.
Get the answer of all your queries regarding IVF from our fertility specialist. To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
Symptoms of breast cancer include a lump in the breast, bloody discharge from the nipple and changes in the shape or texture of the nipple or breast. Redness, swollen lymph nodes, discomfort or thickening or puckering of the skin are also experienced by some people.
Get the answer of all your queries regarding IVF from our fertility specialist. To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
Best infertility hospital in indore, ivf specialist in indore, ivf center in indore, test tube baby center in indore, ivf treatment cost in indore, Best centre for IVF in indore, affordable ivf cost in indore, best fertility hospital in india, best ivf center in mp, infertility treatment in indore, best ivf centre in india, ICSI treatment in indore
The purpose of this study was the analysis of a correlation, in infertile patients, between the quality of the endometrium based on its vascularisation and the chances of conception. Hysteroscopy was carried out to determine the quality of the endometrial surface using the Sakumoto–Masamoto classification (“good” vs. “poor” endometrium) in the secretory phase of the menstrual cycle. The results were set in relation to the outcome of the subsequent infertility treatment, i.e. the establishment of a pregnancy within the study period (4 years). In 108 (67%) of the 162 followed-up patients, the endometrium was endoscopically classified as “good”, while in 54 (33%) the result was “poor”. The overall pregnancy rate was 37% (60 patients); 47 of all pregnancies (78%) occurred in women with a “good” endometrium while 13 (22%) had a “poor” classification. This positive association between the establishment of a pregnancy in the follow-up and a “good” classification of the endometrial vasculature in the group with a “good” endometrium was significant (P = 0.0165, Fisher’s exact test). This study confirms the usefulness of endometrial evaluation by hysteroscopy as a diagnostic instrument for providing a prognosis of the chance for the patients to become pregnant.
Background
One of the most difficult questions put forward by patients after the failure of a fertility therapy such as in vitro fertilisation (IVF) and intra-cytoplasmic sperm injection (ICSI) is related to the lack of success. The implantation rate per transferred embryo normally does not exceed 30%. Often the failure of “embryo implantation” is given as an explanation as the failure in one of the most critical stages at the beginning of conception, i.e. when apposition and implantation has to occur inside the uterine cavity. Current knowledge about the mechanism of these interactions is still difficult to interpret [1].
Various different suggestions have been made for investigating these mechanisms and attempting to understand which would be the characteristic elements of the endometrium that ensure ideal conditions for the embryo; but they have until today been limited to the so-called theory of the endometrial “opportunity window” [2] and did not offer effective clinical instruments for understanding which groups of patients would be at an increased risk of embryo implantation failure [3]. By using hysteroscopy as a diagnostic procedure for the assessment of pathologies inside the uterine cavity, it has, however, been shown that the differential characterisation of the endometrial surface could be a helpful tool for evaluating the in vivo vascularisation of the uterine mucosa. Already, Sakumoto et al. in 1992 in the first place [4], and after him Masamoto et al. in 2000 [5], have described the technique and used this differentiation in order to demonstrate that the endometrium could be classified into two distinct groups: a “good” endometrium, which has circular gland openings and an intense vascular ramification on one hand, and a “poor” endometrium, which is characterised by a surface with a lower gland and vascular density on the other.
The purpose of this study was to demonstrate the impact of the hysteroscopy, according to this vascularisation-based staging, and to investigate whether this endometrium quality could be used as a tool to assess the potential to achieve a pregnancy irrespective of the chosen type of infertility treatment.
Materials and methods
All infertile patients attending our fertility centre and with a regular menstrual cycle were asked to participate in this comparative, prospective study. They underwent a pre-operative transvaginal sonography (TVS), a full hormonal assessment (FSH, LH, 17β-estradiol, thyroid-stimulating hormone and prolactin) in the serum on cycle days 3 to 5 and then a hysteroscopy in the second part of the menstrual cycle for evaluating the vascularisation of the endometrium. Informed, written consent was obtained from the patients after explanation of the study by the clinician prior to the procedure, and they were asked to avoid a pregnancy in the examination cycle. The study protocol was approved by the local ethical committee.
The inclusion criteria were infertility (absence of conception after 12 months of regular, unprotected intercourse), age less than 43 years, regular cycles (25–31 days) and normal hormonal values (including FSH <12 mU/mL) had to be fulfilled. All partners provided a spermiogram for the exclusion of male factor infertility. Further exclusion criteria were known causes of uterine malformations, endometrial adhesions and hormonal therapy such as oral contraceptives or other oestrogen–progesterone medications within the last 3 months before hysteroscopy. If necessary, the procedure was combined with a laparoscopy to test the tubal patency, and the hysteroscopy was done in most cases during the same operating session and under general anaesthesia. The ultrasonographers were located in the same university department, but not involved in the surgical procedure, and the surgeon was blinded to the TVS findings.
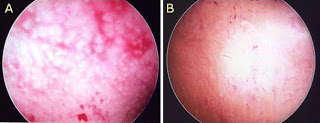
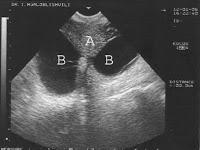
The endometrial surface was evaluated according to the Sakumoto–Masamoto grading (“good” vs. “poor”). Endoscopic findings were categorised as “good” with an appearance representing ring-type glandular openings and maximal glandular secretion or “poor” with a low development level of vessel networks on the endometrial surface. This is illustrated in Fig.1. Hysteroscopic procedures were carried out when indicated (e.g. polyps, myomas, adhesions, septa). The diagnostic hysteroscopy was performed with a 5-mm-outer diameter scope (30°, Karl Storz) connected to a standard endoscopic camera, and a saline solution at low pressure (not higher than 60 mmHg) was used for the distension of the uterine cavity. Hysteroscopic findings were observed and analysed by three gynaecologists using videotape records.
The follow-up interval lasted for 12 months from hysteroscopy. Data were recorded and analysed for a correlation between the vascularisation score of the endometrium and the occurrence of embryo implantation (spontaneous pregnancy, successful outcome after hormonal stimulation with or without intrauterine insemination or successful IVF/ICSI-embryo transfer treatment). For statistical evaluation, the Fisher’s exact test was applied using GraphPad Prism Software (San Diego, USA). For alpha, we considered 0.05 as cutoff value to avoid type I error.
Findings
A total of 178 infertile women underwent a hysteroscopic assessment, and 162 (91%) of them could be followed up in our hospital. A “good” endometrium according to Sakumoto–Masamoto staging was diagnosed in 108 of them (67%), while 54 (33%) patients were graded as “poor”. No differences in the distribution pattern of the causes and duration of infertility, the age of the patients (mean 33.8 years in the “good” and 33.6 in the “poor” group) or the pre-treatment day 3 serum level of follicle-stimulating hormone (6.8 and 7.4 U/L) were observed between these two groups.
A normal uterine cavity was reported in 133 (83%) women, while endometrial polyps, submucosal fibroids, adhesions or uterine malformations were found in 29 cases (17%). On the other hand, the pre-operative TVS indicated intrauterine pathologies in 15 cases (9.3%). The overall pregnancy rate was 37% (60 women); 15 women became pregnant spontaneously, 22 patients succeeded after follicular stimulation with recombinant gonadotropins (rFSH) and 23 after treatment with in vitro fertilisation and embryo transfer including ICSI.
In the total pregnancy group (N = 60), a “good” endometrium was found in 47 women (78%) while this was the case in 61 patients (60%) of the group who did not achieve a pregnancy. Forty-one patients with a “poor” endometrium did not succeed in getting pregnant. Only 13 patients with a “poor” endometrium did succeed in establishing pregnancy in the follow-up. The association between endometrium quality by Sakumoto–Masamoto classification and pregnancy outcome was statistically significant (P = 0.0165, OR = 2.43, CI = 1.17–5.05); the contingency matrix for the pregnancy outcome is shown in Table 1.
Conclusion
Our results confirm those of the studies carried out by Sakumoto and Masamoto [4, 5], indicating that a hysteroscopic examination of the mid-secretory endometrium can be a reliable instrument for determining the chances of a patient to become pregnant. The classification in “good” and “poor” is leading to the conclusion that a poorly vascularised endometrium with limited glandular (secretory) structures may result in a tissue which is not suitable for a correct embryo implantation and endometrial development, and this irrespective of other factors of sterility.
Nevertheless, our results showed a lower fraction of patients (one third) with a “poor” endometrium in comparison to earlier studies (45.9% in the study of Sakumoto [4] and 61.3% in Masamoto et al. [5]): we believe that this difference can be explained with a different patient selection in the study groups. As a matter of fact, we did not focus on patients with a history of repeated abortions as it was the case in the study of Masamoto [5], but on a global infertile population.
Another clearly interesting but only partially surprising finding is the high percentage (17.2%) of intrauterine pathologies that have been diagnosed in the hysteroscopic examination when compared to the total number of patients with suspected intracavitary problems found in the pre-operative sonography (9.3% of all women, and this in spite of all ultrasound examinations having been carried out by the same team of experienced gynaecologists). These results, nevertheless, are in large agreement with previously published studies [6, 7].
We therefore conclude that a hysteroscopic examination, particularly in cases of idiopathic infertility or after several unsuccessful treatment cycles with in vitro fertilisation [8], is strongly indicated [9] and has the added benefit of providing a prognostic measure for determining the chances of the patient to become pregnant, in the future, in addition to its diagnostic significance [10].
Are you looking for the Best IVF specialist in indore? Dr Shilpa Bhandari is one of the first reproductive medicine specialist of this country. She has not only been a pioneering force in the development of an MCI recognized DM/ McH reproductive medicine curriculum, but has also procured this prestigious super specialization by 3 years of extensive training in this field.
She looks after the needs of more than a thousand patients annually in terms of consultation, surgeries, IVF, medical treatment, etc. she has also been actively involved in training other doctors as well as research. She has authored more than 20 research papers in national and international journals. Dr Shilpa Bhandari is an ardent believer in open patient communication, maintaining and honest doctor patient relationship and patient empowerment. Her dream is to provide affordable, honest patient care to couple seeking to enhance their families. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com
There is no reason for a complete restriction on physical activity during IVF. For many women, exercise is a stress relief strategy. Undergoing IVF is a naturally stressful process, and it is important to use all of your resources to reduce anxiety and tension. However, you should keep your exercise routine to a low-impact maximum during the cycle. While mild to moderate exercise is acceptable during IVF treatment, patients should be careful about what types of exercises they perform. Focus on low-impact exercises that encourage stress relief.
It’s also important to drink plenty of water before, during and after a workout, and to eat a healthy and well-balanced diet to keep your energy up. Above all, remember: Taking care of your body should be your top priority during your IVF cycle.
Get the answer of all your queries regarding IVF from our fertility specialist. To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
Best infertility hospital in indore, ivf specialist in indore, ivf center in indore, test tube baby center in indore, ivf treatment cost in indore, Best centre for IVF in indore, affordable ivf cost in indore, best fertility hospital in india, best ivf center in mp, infertility treatment in indore, best ivf centre in india, ICSI treatment in indore
Hypothalamic Dysfunction Excess Physical or emotional stress, a very high or a recent substantial weight gain or loss can disrupt production of certain hormones and affect ovulation.
Get the answer of all your queries regarding IVF from our fertility specialist. To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
One of the intensively discussed topics recently is investigation of infertile patients. A subject of particular interest is a new technique – transvaginal hydrolaparoscopy (TVHL), which has already found its place amongst other methods of infertility exploration. Transvaginal hydrolaparoscopy allows atraumatic investigation of reproductive organs in physiologic conditions, in ambulatory settings. Significant, for clinical practice, is the possibility of a combination of transvaginal hydrolaparoscopy with other methods of investigation – sonohysterosalpinogography, hysteroscopy and salpingoscopy, which make possible integrated exploration of the reproductive system. Instillation of saline into the pelvic cavity through uterine tubes (or through puncture needle if needed) under ultrasonographic control and exposition of posterior fornix, allows better orientation in the pouch of Douglas, complex assessment of reproductive organs and determination of advisability of pelvioscopy – the relatively invasive technique as well as thorough control of the safe access to the pouch of Douglas.
Since Gordts et al. in 1998 have introduced the technique of transvaginal hydrolaparoscopy (TVHL), for the investigation of infertile women [1], interest to the vaginal route of genital tract exploration has been recommenced.
Introduction of more global concept of fertiloscopy: concurrent performance of pelvioscopy, hysteroscopy, salpingoscopy and microsalpingoscopy with chromopertubation [2] allows for an increase in usefulness of infertility investigation and to optimize treatment strategy for infertility management with the consequent saving of time and costs. Introduction of this highly informative endoscopic technique into the format of one-stop investigation of infertility has become possible after the introduction of a new technique of atraumatic access to the pouch of Douglas via vaginal route using new instrumentations for transvaginal hydrolaparoscopy (TVHL) in the ambulatory settings [3, 4].
From April of 2002 till November of 2005 we have performed 837 fertiloscopies. As we described previously [5], TVHL with hysteroscopy and salpingoscopy is routinely performed in our clinic, in complex with sonohysterosalpingography and with extensive use of ultrasonographic control, in order to assess the future diagnostic insertion into the pouch of Douglas, as well as to ensure safety of this manipulation (instillation of warm saline for exposition of the posterior fornix of vagina).
The most difficult stage of TVHL is the introduction of instruments through the posterior fornix of the vagina into the pouch of Douglas. According to the data of various authors, access to the pouch of Douglas failed in 4.3-0% cases [1–4, 6–15]. Complications are expected when the patient has a retroverted uterus or in the presence of ovaries, uterine tubes, leiomyoma, bowel loops or varicose veins in the pouch of Douglas. Some authors consider such disposition as a relative/absolute contraindication to the procedure [1, 3, 4, 7, 12, 14, 16]. According to the data, the bowel trauma took place in 0.65% of procedures, but after the initial experience it has reduced to 0.25[16]. In 50% of cases, bowel injury was estimated by the surgeon as avoidable. The development of safe techniques for insertion of instrument/s into the pelvic cavity, as well as determination of the capability and the necessity of performing pelvioscopy is highly important.
As a matter of fact, nowadays there are several, similar systems of instruments for the access to the pouch of Douglas which differ in construction of the puncture needle (combined needle-trocar system with adapted Veress needle, and separate needle and trocar system). All systems have their advantages and disadvantages, but discussion of these topics is not the aim of this article. We would like to introduce some safe methods which enable the avoidance of complications to a grater extent, and to specify the possibility and rationality (reasonableness) of the performance of TVHL.
During performance of procedures we use Transvaginal hydrolaparoscopic kit (Circon ACMI, Stamford, CT) or Transvaginal hydrolaparoscopy set (Karl Storz, Tuttlingen, Germany). Ultrasonographic investigation/assistance was performed using Aloca SSD 650 with transvaginal probe with a frequency of 5.5 MHz, equipped with the puncture set.
During the process of preparation for laparoscopic investigation, detailed ultrasonography is performed with particular attention to the location of uterine corpus, uterine cervix and vagina, also to the state of posterior fornix of the vagina and the contents of the pouch of Douglas.
The first stage of the investigation is routine hysteroscopy, after which the pouch of Douglas is partially filled with saline (if at least one of the uterine tubes is patent).
The second stage is the routine sonohysterosalpingography during which by transtubal instillation of 60–200 ml of saline into the pelvic cavity, exposition of the posterior fornix of vagina is reached, which makes it possible, against a background of instilled fluid, to clearly visualize and assess the fornix (Figs. 1, 2, 3 and 4 determine the presence, the location and the characteristics of adhesions in the pouch of Douglas, presence of dilated vessels and presenting organs in minor pelvis. (Figs. 5, 6, 7 and 8).
In the case of non-patency of uterine tubes, which makes the instillation of saline into the pelvic cavity impossible, transvaginal puncture set is used under the ultrasonographic control, to allow exposition of the posterior fornix by instillation of water via an aspiration needle Fig. 7. The presence of follicular fluid during ovulation sometimes is quite enough for ultrasonographic orientation in the situation.
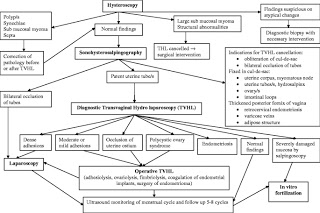
The third stage of investigation is the transvaginal hydrolaparoscopy: an insertion of laparascopic instruments into the pelvic cavity is performed, if there have not been revealed contraindications or reasons of TVHL cancellation (for example hydrosalpinges-Fig. 8) at previous stages of investigation. These conditions are:
Complete obliteration of the pouch of Douglas Fig. 5.
Thickening of posterior fornix, often with uneven echo structure and width Fig. 2, with the visualized dilated vessels Fig. 3, sometimes with presence of retro cervical endometriosis or varicose veins, adipose structure behind the posterior fornix or vagina Fig. 4.
Intensive adhesions in the pouch of Douglas Fig. 7.
Localization of fixed organs of minor pelvis into the pouch of Douglas: one or both ovaries, uterine tube/s Fig. 8, intestinal loops Fig. 5, myomatous node or uterine corpus Fig. 6.
Bilateral hydrosalpinges Bilateral Fig. 8.
Among the investigated 837 infertile women, in 6 cases was detected suspicious pathology on atypical alterations, thus further stages of investigation were postponed until an appropriate differential diagnosis is obtained.
Results of the next stage, sonohysterosalpingography for the remaining 831 women are summarized in Table.
After the stages of hysteroscopy and sonohysterosalpingography, transvaginal hydrolaparoscopy was performed in 702 of the 837 women. An extent of exploration was determined during the procedure, after considering advisability and possible safety of conducting different interventions (Fig. 9 Algorithm of management). In 135 (16.1%) women out of 837 TVHL was cancelled or postponed. We have not noted any complications during performed investigations.
Hydrosalpinges of at least one of the tubes, does not represent contraindication for performing transvaginal hydrolaparoscopy per se (if it is not obliterating the pouch of Douglas), but often on the stage of sonohysterosalpingography/hystreoscopy the need for the transvaginal hydrolaparoscopy vanishes, as a treatment strategy of infertility becomes evident (Fig. 9 Algorithm of management). On the basis of already discovered findings it is possible to switch to the accepted interventions for infertility management. This includes either restoration of natural fertility – reconstructive surgery of the uterine tubes or creation of optimal conditions for IVF (proximal obstruction of tubes, salpingectomy etc) [17].
Ultrasonographic control during procedure of transvaginal hydrolaparoscopy not only allows an evaluation of the proximal parts of tubes which in complex increases informativeness of the investigation, but also gives a possibility to visualize existence of adhesions in the pouch of Douglas-together with the introduction of the trocar system. However it is not sufficient enough to assess the role of adhesions in infertility as this method is not able to access the fimbrial-ovarian area- a key functioning part of the reproductive tract.
Thus, we present the investigation of infertility which includes: hysteroscopy, sonohysterosalpingography with instillation of fluid into the pelvic cavity (if necessary via puncture needle) under ultrasonographic control, which provides exposition of the posterior fornix and orientation in the pouch of Douglas, hydropelvioscopy with dye chromopertubation and salpingoscopy. Such a format of investigation makes it possible for amore complex evaluation of reproductive system and determination of advisability of performance of transvaginal hydrolaparoscopy – a relatively invasive procedure with more intensive control of safety of the access to the pouch of Douglas.
Are you looking for the Best Fertility hospital in India? Mohak Infertility Center is one of the leading Best Fertility hospitals and Test tube baby center in indore Mohak Infertility Center is a IVF center in Indore Madhya Pradesh with an excellent and experienced team of IVF specialist and embryologists, who are able to offer you today’s most advanced and effective procedures in IVF treatment. Our IVF Specialists and embryologists have been trained and have worked in some of the Best IVF Centers of the world, Mohak Infertility Center in Indore aims to give you the best chance of having a healthy baby. Our team of IVF specialist and support staff is committed to provide you the best possible care and advise that you can trust. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com
Feeling Emotions and Overthinking — mental health playing important role in reproductive hormone regulation if we are stressed it may affect to conceive a baby.
Get the answer of all your queries regarding IVF from our fertility specialist. To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com