Abstract
Transvaginal hydrolaparoscopy is a culdoscopic approach for the inspection of the posterior pelvis, but, in contrast to culdoscopy, uses an aqueous solution for the distension of the pelvic cavity and small diameter optics. The technique is used for diagnostic purposes in patients with infertility and is performed under local anesthesia or conscious sedation in an ambulatory surgical center. We report on a continuous series of 1,000 patients with infertility and without obvious pelvic pathology. Access and good visualization was obtained in 96.8% of the patients. The main complications were intraperitoneal bleeding and bowel perforation, which after the initial period occurred respectively in 1.9 and 0.1%. All complications were managed conservatively, and no major complication occurred. Clinically significant pathology was diagnosed in 25% of the patients, which allowed immediate triage of the patients for further management. Transvaginal hydrolaparoscopy can be proposed as a first line technique to replace hysterosalpingography and diagnostic laparoscopy in the exploration of patients with unexplained infertility.
Introduction

In Europe over the past 40 years, endoscopic evaluation of the pelvis has become an integral part of the infertility work-up. In routine practice, hysterosalpingography (HSG) is the first-line investigation and, if normal, laparoscopy is frequently delayed for 6 months or more. Laparoscopy is indeed an invasive procedure, associated with potentially serious complications, and together with hospitalization it can also be an expensive procedure. On the other hand, HSG is inferior to the chromopertubation test for the diagnosis of tubal patency [1] and also has a low sensitivity for the diagnosis of pelvic endometriosis and adhesions. If laparoscopy is performed as a first-line investigation on all infertile patients, there will be a large number of patients with normal findings or with minor pathology that has no or doubtful impact on the management of infertility.
It has been argued that with the advent of ART, laparoscopy can be omitted from the infertility work-up when there is no abnormal contributing history and the HSG is normal and, as a consequence, the cost of fertility treatment is reduced without compromising success rates [2]. Karande et al. [3], however, found in a prospective randomized trial that a higher pregnancy rate with lower costs is achieved with a traditional treatment algorithm than with IVF-embryo transfer as a first line-therapy.
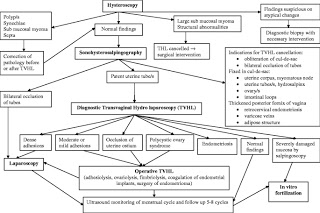
We therefore wish to report on a continuous personal (H.V.) series of 1,000 procedures of transvaginal laparoscopy (THL), which were performed in combination with the mini-hysteroscopy and chromopertubation test as a first-line investigation of female infertility [4]. The combination of the three procedures has been coined transvaginal endoscopy (TVE).
Materials and methods
THL was discussed with all women who met prospectively established exclusion and inclusion criteria. In all patients, the indication was primary or secondary infertility. The patients had a complete history, physical examination and transvaginal sonography. Patients were excluded if they had an indication for operative laparoscopy, abnormal pelvic findings such as fixed retroverted uterus, rectovaginal endometriosis, large ovarian cyst or obliterated cul-de-sac, or an upper vaginal stenosis. Patients with vaginal or pelvic infection were first treated before THL was performed.
THL was used as described by Gordts et al. [5]. With the patient in the dorsal decubitus position, only a limited amount of fluid is required to have the tubo-ovarian structures floating in the excavation of the posterior pelvis. We used a narrow-diameter (<3.5 mm), foroblique 30°, wide-angled and rigid optic, a high intensity light source and a digital camera. Inspection of the pelvic structures was achieved without grasping or manipulation. At the end of the procedure a chromopertubation test was performed and, when indicated, salpingoscopy was added. All interventions were performed under conscious sedation as an office procedure in an outpatient surgical suite.
Transvaginal laparoscopy was considered complete if the tubo-ovarian structures, pelvic sidewalls and cul-de-sac could be seen, or if pathology was diagnosed that indicated the need for operative intervention or ART.
Results
A total of 1,000 THLs were performed during the period starting from 1998 until 2003. Thirty-two (3.2%) failures occurred with failed access in 11 (1.1%) and absent or poor visualization in 21 (2.1%). In total, 968 (96.8%) of the procedures were completed. No pathology or pathology of minor clinical significance was found in 736 (76%). In the group with completed procedures, unexpected clinically significant pathology was diagnosed in 240 (25%) and included mainly ovarian endometriosis, tubo-ovarian adhesions, isthmic block and hydrosalpinges. The diagnostic findings resulted in 36 (3.7%) operative laparoscopies and 204 (21.1%) medical therapies and ARTs.
No major complication occurred in this series. Intraperitoneal bleeding was seen in 23 (2.3%) of the patients and occurred on the posterior wall of the uterus (n=13), parametrium (n=2), ovary (n=2), omentum (n=1) and adhesions (n=5). Bowel perforation occurred in 5 (0.5%) and was managed conservatively with antibiotics. Infection occurred in two (0.2%).
The correlation of the failures (no access or no visualization) with the experience showed that 5 (10%) failures occurred in the first 50 procedures and 26 (2.8%) in the subsequent 950 procedures (P=0.018). Bleeding occurred in 5 (10%) of the first 50 cases and 18 (1.9%) of the following 950 cases (P=0.004). Bowel perforation occurred in 4 (8%) of the first 50 cases and in 1 (0.1%) of the following 950 cases (P<0.0001).
Discussion
By using TVE as a first-line investigation of female infertility, we avoided HSG in 96.8% and laparoscopy in 93.2% of the patients. In 24% of the patients, unexpected major pathology was diagnosed and recommendations for operative laparoscopy, medical therapy or ART could be made.
Several studies have validated the feasibility, reproducibility, diagnostic accuracy, acceptability and safety of the procedure [6]. Different centres have reported access in over 95% and normal findings in 41 to 59% of the cases. In this series of 1,000 consecutive cases, access and visualization of the pelvic structures were achieved in 96.8% of the patients. The performance of THL is defined by visualization of the ovaries, fallopian tubes, posterior wall of the uterus, ovarian and uterosacral ligaments, sidewall of the posterior pelvis and cul-de-sac. In this series, these structures were normal or showed pathology of minor significance in 76% of the patients.

The potentially serious complication of transvaginal access is rectal perforation and sepsis. In a survey of 3,667 procedures the incidence of bowel perforation was 0.65%, which decreased after the initial experience to 0.25%. No delayed diagnosis and sepsis occurred, and 92% of the cases were managed with outpatient antibiotics [7]. In the present series minor bleeding occurred in 2.5% and bowel perforation in 0.5% of the patients. Analysis of the occurrence of complications in function of experience confirmed the importance of the learning curve. After the initial 50 cases, the complication rate of intraperitoneal bleeding and bowel perforation decreased significantly to 1.9 and 0.1%, respectively. It should, however, be noted that even in experienced hands these complications can occur and, therefore, the patients need to be informed. However, in this series no major complication such as sepsis occurred and, similar to previous series, most bowel perforations were managed conservatively with antibiotics without consequences.
As a first-line procedure for the investigation of female infertility, TVE is in direct competition with HSG. The prognostic value of the chromopertubation test has been shown to be better than that of HSG [1]. Four authors reported abnormal findings at THL in 44% of 241 patients with normal or suspected hysterosalpingography [6]. Shibahara et al. [8] compared HSG versus THL in a series of patients with and without a history of Chlamydia infection and found that THL was superior for the diagnosis of peritubal adhesions. The additional advantage of THL for tubal exploration is the ability to examine directly the tubal mucosa by salpingoscopy. Salpingoscopy is a better predictor for pregnancy outcome after tubal reconstructive surgery than routine investigation by HSG and standard laparoscopy [9, 10].
Fatum et al. [2] suggested that in patients with a normal HSG, laparoscopy would be superfluous and patients should undergo up to six cycles of gonadotropins and IUI and then undergo IVF if they continue to be infertile. However, in a recent study Capelo et al. [11] found significant pelvic pathology in one third of the patients failing to conceive after four ovulatory cycles of clomiphene citrate and concluded that early endoscopic diagnosis of such pathology would have allowed the couple to proceed directly to IVF.

Cicinelli et al. [12] found in a randomized controlled trial that THL in combination with mini-hysteroscopy in an outpatient setting was better tolerated by the patients than HSG. Finally, HSG is a diagnostic X-ray procedure that exposes the bladder, ovary and colon to radiation. The organ-specific radiation doses of HSG for the bladder and colon are estimated at 4.67 and 2.82 mGy, respectively. It is now generally accepted that there is no threshold dose below which radiation exposure does not cause cancer, and the attributable risk of diagnostic X-rays is estimated to range from 0.6 to 1.8 of cases of cancers per year [13].
When an accurate infertility exploration can be performed with a minimally invasive procedure and a reliable treatment exists, an early diagnosis followed by the most appropriate, effective treatment can greatly reduce the monthly failures and the sense of frustration for the couple, particularly when age and time are additional unfavorable factors
Our current approach of exploring female fertility after 1 year or more of infertility may paradoxically lead to undertreatment as well as overtreatment.
Recent prospective population-based studies have demonstrated that the time to clinical pregnancy in most women with normal fertility is not more than 6 months [14, 15]. It can therefore be assumed that already after six cycles with fertility-focused intercourse, irrespective of their age, most women with normal fertility have conceived and that the remaining group is largely composed of couples faced with subfertility. Today, when female fertility can be explored accurately with a minimally invasive procedure, such as TVE [4], and a reliable treatment exists for many major disorders, a prolonged waiting period is outdated.
It is concluded that in women with previously normal cycles infertility should be investigated already after a 6-month period of fertility-focused intercourse and that transvaginal endoscopy, which combines minihysteroscopy and transvaginal hydrolaparoscopy, can be proposed as a first-line technique.
fter a 6-month period of fertility-focused intercourse and that transvaginal endoscopy, which combines minihysteroscopy and transvaginal hydrolaparoscopy, can be proposed as a first-line technique.
Source – https://gynecolsurg.springeropen.com/articles/10.1007/s10397-004-0030-3
Mohak Infertility Center is a one of the Best fertility hospitals in india. At the Mohak Infertility Center, We provide treatment of infertility by latest techniques for assisted conception and reproduction. Providing ICSI Treatment in indore at reasonable cost with best way to improve results. Get the best infertility treatment in indore at Mohak Infertility Center with complete infertility care at low cost. Book an appointment Today Call now 7898047572 For more information, visit – https://www.mohakivf.com

Please go through our social media :
like our page to no more about ivf
Facebook : https://www.facebook.com/MOHAK-IVF-1167147806785287/
Please do follow on Instagram
Instagram : https://www.instagram.com/mohak_ivf/
To More Post: Hysterosalpingography in the workup of female infertility: indications, technique and diagnostic findings