Feeling Emotions and Overthinking — mental health playing important role in reproductive hormone regulation if we are stressed it may affect to conceive a baby.
Get the answer of all your queries regarding IVF from our fertility specialist. To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
Get the answer of all your queries regarding IVF from our fertility specialist. To book an appointment Call 78980–47572 / 80852–77666 or For more detail visit www.mohakivf.com
Tubal factor infertility accounts for approximately 25–35% of cases of female infertility [1–3]. Identifiable causes of tubal infertility are postinfectious tubal damage, post surgical adhesion formation, and endometriosis-related adhesions.
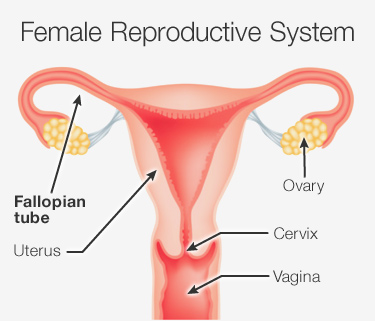
The normal process of captation of the oocyte requires a series of prerequisites: the ovarian surface free from adhesions, the fimbrial-ampullary portion of the tube free to embrace the ovary and, beside tubal patency, a normal activity of the ciliated and secretory cells of the tubal mucosa. Furthermore, the muscular layer of the tube must be undamaged and able to contract.
In recent years the treatment of tubal infertility has witnessed a shift from tubal reconstructive surgery to in vitro fertilization–embryo transfer techniques (IVF). Due to the wider availability of assisted reproductive technologies, the number of women with mechanical infertility treated by reconstructive surgery has decreased, most couples being referred to IVF.
Reproductive surgery is performed with the aim of allowing ovum pick-up by restoring normal anatomic relationships between the fimbriae and the ovary. However, even though reproductive surgery may be successful in restoring normal anatomy, it may not be able to restore normal function of the damaged tubal mucosa.
The percentages of success of the surgical treatment are therefore strictly correlated with the type of preexisting tubal damage, independently of the surgical technique performed.
Recent refinements of laparoscopic instrumentation and increased surgical skills in operative laparoscopy allow laparotomy to be avoided in most instances.
The advent of salpingoscopy, a technique that allows direct visual evaluation of the tubal mucosa, has allowed improved selection of patients who are candidates for tubal reconstructive surgery by identifying the patients with good reproductive prognosis. The following is an analysis of the various indications to tubal surgery according to the level (proximal or distal) and type of tubal pathology.
Proximal tubal occlusion (PTO) Lack of passage of the contrast medium at the level of the intramural–isthmic portion of the fallopian tube during an hysterosalpingogram (HSG) or a laparoscopy with chromopertubation may be due to a true occlusion consequent to postinfectious fibrosis or to an obstruction due to technical artifacts, a spasm of the uterine tubal ostium, a valve mechanism determined by an area of endometrial thickness (focal hyperplasia), or to plugs of amorphous material.
Bilateral PTO is a relatively infrequent finding. We reported [4] that out of 665 patients undergoing laparoscopy with chromopertubation for primary or secondary infertility, only 35 patients (5%) had bilateral PTO confirming a previous HSG finding (25 patients bilateral, 10 unilateral with the contralateral tube either distally occluded or absent). Of these patients, 17 refused any further treatment. After a mean follow-up of 25 months, 3 (18%) of these patients spontaneously conceived an intrauterine pregnancy; 4 out of 5 patients who underwent a repeated HSG had bilateral tubal patency. Therefore, the diagnosis of bilateral tubal occlusion proved to be incorrect in 7 out of 17 patients (42%).
Furthermore, with regard to the etiology of temporary proximal tubal obstruction, a recent paper [5] hypothesizes that small air bubbles, but more likely tubal kinking, may be an explanation of these findings in the patients undergoing HSG in the supine position. In a series of 156 patients, unilateral PTO was diagnosed in 15% of patients (24 of 156) and bilateral PTO in 3% (4 of 156). Rotating the patient such that the obstructed tube was inferior to the uterus resolved 63% of the unilateral PTO, likely by unkinking the tube at the uterotubal junction, thus dramatically lowering the resistance to the flow of contrast medium. The same manoeuvre was less effective in bilateral PTO, where 25% of the more dependent tubes became patent. Still, this report offers an important contribution to the explanation of “reversible” PTO. The possibility that some PTO are obstructions and not true occlusions is supported by the study of Sulak et al. [6] who in 1987 reported on 18 patients who were found to have bilateral PTO by both HSG and subsequent laparoscopy with chromopertubation and therefore underwent resection of the occluded tubal segment and anastomosis. Resected tubal segments were studied histologically, and in 11 of the 18 cases no tubal occlusion could be demonstrated. In six cases (three with occlusion and three with apparent patency) the tubal lumen contained an amorphous material of unknown etiology, often appearing to form a cast of the tube. The authors were the first to report on such “plugs” and speculated that, if they cause tubal obstruction, this would explain previously published findings of high pregnancy rates in infertility patients after HSG. The suggested mechanism would be, among others, dislodging of tubal mucus plugs.
In 1987 Thurmond et al. [7] described their technique for selective salpingography and fallopian tube recanalization that has since then been widely used to improve diagnosis by injecting contrast medium through a catheter placed in the tubal ostium. This technique allows differentiation of tubal spasm from true occlusion, and can be performed in the same session as the hysterosalpingographic examination that fails to opacify the tubes. In fallopian tube recanalization, a catheter and guide wire system is used to clear proximal tubal obstruction by amorphous debris.
A review [8] evaluating results with this technique in 1,466 patients reports a successful recanalization of the proximal fallopian tube in 71–92% of recanalization attempted. Pregnancy rates after the procedure have been variable among series, with an average rate of 30% during follow-up.
In a retrospective study, Al-Jaroudi [9] et al. have recently evaluated the reproductive performance of women after selective tubal catheterization. Ninety-eight infertile women with hysterosalpingographic findings of PTO underwent a repeat hysterosalpingography examination before selective tubal catheterization. Bilateral tubal patency was documented in 14 patients and patency of one of the tubes in 12 others. PTO was confirmed in 72 patients. Successful recanalization of both tubes was achieved in 25 patients (34.7%) and successful recanalization of at least one tube was achieved in 44 patients (61.1%). Of the 72 patients who underwent selective tubal catheterization, 23 conceived (31.9%). The cumulative probability of conception was 28%, 59%, and 73% at 12, 18, and 24 months of follow-up, respectively. The few patients with failure of tubal recanalization may likely have true occlusion caused by fibrotic scarring of the tube from salpingitis, endometriosis, or surgery. Microsurgical resection and tubocornual anastomosis continue to be the standard of care in these cases [10]. In a review of nine case series including 187 patients with PTO, we reported [11] a 49% term pregnancy rate per patient, with a 4% risk of ectopic pregnancy after microsurgery by laparotomy.
In 1987, Patton et al. [12] reported on a series of 27 patients with a postpelvic inflammatory disease (PID) bilateral PTO or PTO of the single remaining tube diagnosed both at HSG and laparoscopy with tubal perfusion. Patients were not excluded on the basis of age, extent of tubal disease, duration of infertility, tubal length, or history of prior operation. After an extended follow-up (mean 1,714 days) the possibility of conception was of 46%, 65%, and 69.3% within 1, 2 and 3 years from surgery, respectively.
The probability of a conception resulting in a live birth was 27%, 47%, and 53.2% at 1, 2, and 3 years after surgery, respectively. When only patients who did not have a previous surgery for infertility were considered, the conception rate was 75% with a live birth rate of 58% after 3 years.
Periadnexal adhesions In case of periadnexal adhesions, the classic open-abdomen surgery has been completely replaced by laparoscopic surgery, because it obtains the same results in terms of reproductive outcomes with all the advantages of the laparoscopic approach (better cosmetic result, minor postoperative pain, shorter hospital stay, decreased risk of postoperative infections, quicker return to work).
The intrauterine pregnancy rate reported in the literature after laparoscopic salpingoovariolysis in nonselected patients ranges from 51–62%, and the ectopic pregnancy rate ranges from 5–8% [10].
Recent prospective studies have demonstrated that the most important prognostic factor in terms of reproductive outcome after reproductive surgery is the status of the tubal mucosa as evaluated by salpingoscopy [13–16]. For salpingoscopy, a 2.8-mm rigid salpingoscope that allows a detailed vision of the tubal ampullary mucosa is used. The salpingoscope is introduced into the abdominal cavity through the operating channel of the laparoscope. The abdominal ostium of the tube is identified and cannulated, and the tubal mucosa is evaluated. At the ampullary level four or five major folds are noted, with minor folds interspersed between them.
The status of the tubal mucosa is classified according to the classification proposed by Brosens et al. [13] as follows: grade I—normal mucosal folds are seen; grade II—the major folds are separated and flattened but otherwise normal (might be considered a grade I distended by increased intraluminal hydrostatic pressure); grade III—focal adhesions are seen between the mucosal folds; grade IV—extensive adhesions are present between the mucosal folds and/or disseminated flat areas are noticed; grade V—there is a complete loss of the mucosal fold pattern.
Grades I and II identify a normal mucosa; grades III to V identify a tubal damaged by a previous pelvic infectious disease.
It has to be stressed that there is no correlation between the score of periadnexal adhesions and intraluminal damage.
Salpingoscopy allows the identification of the patients with normal tubal mucosa who may most benefit from laparoscopic salpingoovariolysis, with a term pregnancy rate of 70%. Data from Brosens and Marana [14–16] indicate that about 80% of patients with periadnexal adhesions have a normal tubal mucosa. Therefore, 80% of the patients with periadnexal adhesions have a normal mucosa, with 70% chance of a term pregnancy after a laparoscopic salpingoovariolysis. Most of the pregnancies occur within 1 year of surgery.
Distal tubal occlusion (DTO) Salpingoneostomy utilizing microsurgical techniques, first described by Swolin [17] in 1967, has been for years the procedure for the treatment of distal tubal occlusion. In a literature review of 14 series, including 1,275 patients, we reported [18] a cumulative intrauterine pregnancy rate with microsurgical salpingoneostomy by laparotomy of 326/1275 (26%). The cumulative term pregnancy rate was 239/1158 (21%), the cumulative spontaneous abortion rate 54/1125 (5%), and the cumulative ectopic pregnancy rate 96/1245 (8%). Ten studies, including 1,128 patients, had complete information on pregnancy outcomes. The cumulative pregnancy rate per patient was 371/1128 (33%). Of the pregnancies, 77% (284/371) were intrauterine, 61% (227/371) were term pregnancies 15% (55/371) were spontaneous abortions, and 23% (87/371) were ectopic pregnancies.
A recent review evaluated five nonrandomized control studies that compared laparoscopic and open microsurgical tubal surgery for treatment of DTO [19]. No significant difference was observed in the intrauterine pregnancy rate between the two groups (laparotomy group: 138/478, 28.9%; laparoscopy group: 104/336, 30.9%; combined OR 1.32 [95% CI 0.58–3.02]). In three of the studies, sufficient information was given to compare surgical techniques used at different stages of tubal disease.
Overall, there was no significant difference in the intrauterine pregnancy rate in laparatomy versus laparoscopy in mild tubal disease (laparotomy group: 83/253, 32.8%; laparoscopy group: 96/243, 39.5% OR 1.06 [95% CI 0.42–2.70]).
For patients with severe stage tubal disease, there was a significantly increased intrauterine pregnancy rate in the laparotomy group (47/210, 22.4% versus 6/86, 6.98%, OR 2.88 [95% CI 1.16– 7.16]).
Subsequently, the principles of microsurgery were introduced in the laparoscopic approach for the treatment of distal tubal disease.
Several classifications have been proposed in order to identify the patients that may most benefit from tubal reproductive surgery in DTO. Various parameters are considered, such as the type and extension of periadnexal adhesions, the degree of tubal occlusion, and the status of the tubal mucosa.
In 1988, the American Fertility Society proposed a scoring system in order to allow the comparison of results obtained from different authors. This was based on the following parameters: type and extension of the adhesions and, in addition, for the classification of distal tubal occlusion, thickness and rigidity of the tubal wall, distal ampullary diameter, and the percentage of mucosal folds preserved at the neostomy site. The importance of intraoperative salpingoscopy to visualize the entire length of the ampullary mucosa was recognized. However, salpingoscopic findings were not included in the scoring system as salpingoscopy was being practiced in very few centers.
Numerous prospective studies have recently demonstrated that, also in the case of distal tubal occlusion, the most important prognostic factor is represented by the status of the tubal mucosa. It is therefore important to identify the patients with normal tubal mucosa by means of salpingoscopy.
In fact, prospective studies have demonstrated that patients with normal tubal mucosa (grades I and II) will have a term pregnancy rate of 65% after salpingoneostomy (compared to 25% obtained in nonselected patients).
Studies of Brosens and Marana [14–16] report that in cases of distal tubal occlusion, the percentage of patients with normal tubal mucosa range from 35–45%. Therefore, in cases of DTO, 35–45% of the patients have a normal tubal mucosa, with a 65% chance of a term pregnancy rate after a laparoscopic salpingoneostomy. Most of the pregnancies occur in 12–18 months.
In conclusion, based on these findings, in cases of DTO, our current approach would be a diagnostic laparoscopy with salpingoscopy. Laparoscopic salpingoneostomy would then be performed in the patients with normal tubal mucosa.
Reversal of tubal sterilization Tubal sterilization is one of the most used contraceptive methods around the world. It has been reported that about 1% of the patients undergoing this procedure subsequently request a reversal of tubal sterilization.
Tubo-tubal anastomosis is best performed with microsurgical techniques by laparotomy. The precision afforded by this procedure allows precise excision of the occluded segments and exact approximation of each layer of the proximal and distal portions of the tube.
As in the majority of cases the tubal segments are normal, the outcome is an anatomically and physiologically normal tube although slightly shorter.
This leads to a high intrauterine pregnancy rate with a low risk of ectopic pregnancy. Gomel and McComb [10] have reported a cumulative intrauterine pregnancy rate of 70% in patients who are <35 years of age and a 55% rate in patients who are 35 years of age or more at the time of reversal, with most pregnancies occurring within 18 months after surgery. The ectopic pregnancy rate is approximately 2%.
Recent improvements in laparoscopic microsurgical instrumentation have prompted a few centers to propose tubal anastomosis by laparoscopic access. In a retrospective clinical study, Yoon et al. [20] reported on 202 women who desired reversal of tubal sterilization. In these patients tubal anastomosis was performed by laparoscopy. The cumulative pregnancy rate in the 186 patients for whom follow-up data were available was 60.3%, 79.4%, and 83.3% at 6, 12, and 18 months after surgery, respectively. Five patients (3.2%) had ectopic pregnancies; one of these patients subsequently conceived an intrauterine pregnancy.
The authors concluded that laparoscopic tubal anastomosis is less invasive and could be an alternative to the procedure by laparotomy.
Gomel and McComb [10] contend that the mechanical disadvantages inherent in laparoscopic surgery will lead inevitably to less precision than that readily attainable by microsurgery by minilaparatomy for any given surgeon. At present there are no randomized trials with sufficient number of patients to answer this question. IVF results According to the American Society for Reproductive Medicine/Society for Assisted Reproductive Technology Registry published in 2007 [21], reporting the results of 79,042 IVF cycles (with and without ICSI) performed in 2001, the percentage of clinical pregnancy was 32.8% per initiated cycle, 38.2% per retrieval, and 40.6% per transfer. The delivery rates were, respectively, 27.2%, 31.6%, and 33.6%. The cancellation rate was 14.1%; the clinical pregnancy loss was 17.2% and the ectopic pregnancy rate 1.8%.
Of the deliveries, 64.1% were singletons, 32.0% were twins, 3.7% were triplets, and 0.1% were greater than triplet deliveries.
According to the European Society of Human Reproduction and Embriology Registry published in 2007 [22], reporting the results of 365,000 ART cycles performed in 2003, the clinical pregnancy rate per retrieval and per transfer were, respectively, 26.1% and 29.1% for IVF, whereas they were 26.5% and 28.7%, respectively, for ICSI. Incomplete data were available for the analysis per cycle and for term deliveries.
Of the deliveries, 76.7% were singleton, 22.0% were twins, and 1.1% triplets.
The latest results published by the North American and European societies reported here confirm a trend toward better results for assisted reproductive techniques with passing years. The same improvements are not present for the results of tubal surgery. A major improvement with this respect has, however, been made in the field of better patient selection for tubal surgery, following which, for example, as previously discussed, a global 25% pregnancy rate in nonselected patients with DTO can be brought up to 65%. In the final section of this review, a personal view on the comparison between IVF and tubal surgery is reported.
Discussion It is important to underline that while IVF is a ‘palliative’ technique, which means that it does not eliminate the problem but bypasses it, surgery is curative in the favourable cases with normal tubal mucosa. This allows women to obtain pregnancy naturally, and it is therefore an option for couples with ethical and religious concerns. If successful, surgery allows women to have more than one pregnancy without further treatment, with an abortion rate similar to that of the normal population.
Indications to IVF for ‘tubal factor infertility’ may not be correct as this diagnosis often proves to be fallacious. In fact, we have demonstrated that the diagnosis of PTO has a high false positive rate due to technical problems, valve mechanism, intraluminal debris, or chronic inflammation. The diagnosis of DTO, although generally accurate, may sometimes be mimicked by ampullary diverticulae, due to a congenital defect of the myosalpinx, that do not need reconstructive surgery and are not incompatible with pregnancy [23].
In a recent study, Hennelly et al. [24] sent a questionnaire to each patient who was known to have delivered an infant after an IVF or ICSI treatment at their university-based assisted reproduction unit and who had not returned for further therapy. Five hundred fifty questionnaires were sent out. Five hundred thirteen (94%) responses were received and analyzed. One hundred six (20.7%) of the 513 respondents reported that they had had a subsequent spontaneous pregnancy. All the pregnancies occurred within 2 years of the IVF/ICSI pregnancy success. The authors underlined that patients entered the program only if they had a valid indication for IVF/ICSI. These patients truly undertook IVF as a last resort. Therefore, it was surprising to find that 19 out of 128 patients with a diagnosis of tubal factory infertility (14.8%) later conceived spontaneously.
With respect to financial concerns, it should be considered that, unlike in the USA, in Italy as in other European countries, operative laparoscopy, even for infertility, is fully subsidized by the government health service when performed in a public hospital. On the contrary, IVF is mainly performed in private centres and is not reimbursed either by the government or private insurances.
The risks of tubal surgery are very low and are due to the known complications of anesthesia and surgery. Although low, the risk of complications is present even in IVF, with a reported prevalence of serious cases of ovarian hyperstimulation syndrome of 14 per 1,000 women after the first cycle and 23 per 1,000 after a mean of 3.3 treatments in the 9,175 patients followed by the National Research and Development Centre of Finland [25].
With regard to cumulative pregnancy rate after IVF, in a recent paper Sharma et al. [26] reported a cumulative live birth rate of 66% following four cycles of IVF. However, the discontinuation rate was very high during the study. Only 36% of patients continued treatment after the first unsuccessful attempt (dropout rate 74%); the dropout rate was 61% after the second attempt, and 69% after the third attempt.
Lack of success and psychological stress are the main factors in influencing the decision to discontinue treatment with increasing number of attempts [27]. A prospective, cohort study reported that an unexpectedly high percentage of couples who performed IVF discontinued the subsidized treatment before the three cycles that were offered. The majority of these discontinuations were due to psychological stress [28].
Concern has recently been expressed about the health of the children conceived after IVF [29, 30]. It has been reported in singleton ART infants a two-fold increase in risk of perinatal mortality, low birthweight, and preterm birth, about a 50% increase in small for gestational age, and a 30–35% increase in birth defects [31]. The same Centre for Child Health Research evaluated all papers published by March 2003 with data relating to the prevalence of birth defects in infants conceived following IVF/ICSI compared with spontaneously conceived infants [32]. Meta-analyses of seven reviewer-selected studies and of all 25 studies identified as suitable for inclusion in a meta-analysis suggest a statistically significant 30–40% increased risk of birth defects associated with ART. The authors conclude that this information should be made available to couples seeking ART treatment.
The guidelines recently approved by the Genetics Committee and the Reproductive Endocrinology and Infertility Committee of the Society of Obstetricians and Gynecologists of Canada for counselling of Canadian women using ART recommend: pregnancy achieved by IVF with or without ICSI are at higher risk for obstetrical and perinatal complications than spontaneous pregnancies; singleton pregnancies achieved by ART are at higher risk than spontaneous pregnancies for adverse perinatal outcomes, including perinatal mortality, preterm delivery and low birth weight; ART has a significant risk of multiple pregnancies; risks of multiple pregnancies include higher rates of perinatal mortality, preterm birth, low birth weight, gestational hypertension, placental abruption, and placenta previa; and that further epidemiologic and basic science research is needed to help determine the etiology and extent of the increased risks of congenital abnormalities associated with ART [33].
An increased risk of congenital malformations in relation to IVF even in singleton infants has been confirmed by a recent review analysing the medical literature update to 2006 [34]. In conclusion, in spite of the recent improvements in the success of IVF, tubal reconstructive surgery remains an important option for many couples. In referral centers, surgery should be the first line approach for a correct diagnosis and treatment of tubal infertility. The success of the surgical treatment depends on careful selection of patients using appropriate diagnostic techniques.
Are you a childless couple frantically searching the Best IVF center in India with Highest IVF success rate? If yes, Mohak Infertility Center is one of the Best Infertility hospitals and IVF centers in indore. Provides you International Standard Infertility Treatment in indore along with assisted reproductive technologies like IUI, IVF, ICSI ,etc at affordable IVF treatment / Test tube Baby Treatment cost along with the satisfaction of being consulted by the most renowned IVF specialist in Indore. it requires of you. Book an appointment Call now 7898047572 For more information, visit – https://www.mohakivf.com
Once you choose hope, anything is possible.. IVF being the most effective way, helped out from problems coming on the way of becoming parent. Hope is something which keeps everything alive so as a new one in our life. why to think we cant have child. In this new world, IVF is the solution. We don’t only give Hope but also help couple to make it possible.
— — — — — — — — — — — — — — — — — — — — — — — — — — — — — — — Book an Appointment Now Call 78980–47572 / 80852–77666 For more detail visit www.mohakivf.com
The IVF technology or Test tube baby is the most advanced and highly recommended assisted reproductive technology. Visit Mohak IVF Center when you are looking for a highly equipped IVF centre with all modern and world-class facilities. Mohak IVF is one of the Best Test Tube Baby Centre in Indore, Madhyapradesh.
Having India’s most renowned doctors and with their experiences, Mohak IVF has managed to register itself in the list of best Test tube baby centres in India. Here in Mohak IVF, you will get International Standard Infertility Treatment and assisted reproductive technologies like IVF, ICSI, IUI, etc. as well as the satisfaction of being consulted by the experienced and renowned specialists in the field of IVF technology.
Mohak IVF centre is not only a common name for the couples looking for Test tube baby centre in Indore or India, but it has also become the preference of couple looking for fertility treatment from all across the world. Being one of the most trusted IVF centres in Indore and in India as well, we are known for providing international treatment standards in the field of infertility treatment as well as assisted reproductive technologies.
We understand that infertility or subfertility condition can be one of the most stressful situations a couple may face. It can be something which can affect you emotionally, physically and sometimes financially as well. At Mohak IVF, we believe in providing the most comfortable treatment by working closely with the patient. In every phase of the treatment, we take care of all the queries of the patient.
Mohak laparoscopy and infertility centre which was established in 2010, is located in the heart of India – Indore. It is a part of a multispecialty advanced care facility. At Mohak IVF, we have fertility professionals who have got their additional education in the fields of medical or surgical remedy for infertility. Our fertility experts devote their full attention and make sure to provide the best possible infertility treatment. We are proud to have Dr Shilpa Bhandari, one of the first reproductive medical specialists of India with us at Mohak IVF centre. She has done her “Doctorate of medicine” (DM) in the field of reproductive medicine and ensures the quality of treatment provided to each patient who visits the clinic under her supervision.
Reach us for your all types of fertility-related issues, we ensure you to provide you with the best infertility treatment.
Are you looking for the Best Test tube baby center in indore? Mohak Infertility Center is one of the Best Test tube baby center and infertility treatment in indore, Madhya Pradesh. The Centre was established in the year of 2011. Mohak Infertility Center is known for its various services covering Infertility assessment, In Vitro Fertilization (IVF), Intra Uterine Insemination (IUI), Intracytoplasmic Sperm Injection (ICSI), test tube baby treatment and infertility treatment. Don’t wait in a queue, book an instant appointment online with Mohak Infertility Center on https://www.mohakivf.com
Let’s win it, together with “IVF”. IVF is the better way to solve your fertility problems
We at Mohak IVF Center Indore provides you best quality IVF treatment with a high success rate at affordable price. Our goal is to make your parenting dreams come true.
Book an Appointment Now Call 78980–47572 / 80852–77666 For more detail visit www.mohakivf.com
Test tube baby or a baby born with the help of assisted reproductive technology is very common these days. IVF or In vitro fertilization is known as the most common and useful type of assisted reproductive technology which helps women become pregnant. In this technology (IVF), an egg is fertilized outside the woman’s body, i.e., in a laboratory dish. The next process is implantation of the fertilized egg inside a woman’s uterus.
IVF or In vitro fertilization has been used since the late 1970s. It is always done under the supervision of highly experienced doctors and staffs. It involves the use of high-end medical devices and in technically equipped centres. Mohak IVF is one of the best IVF centres across India with all the world-class facilities and highly experienced doctors. There might be specific differences in techniques depending on the clinic, but In vitro fertilization usually involves steps listed below:
1. Natural menstrual cycle suppression
A drug is injected in the form of a daily injection for about two weeks which suppress the natural menstrual cycle.
2.Superovulation
FSH, which makes the ovaries produce more eggs in comparison to usual, is given to the woman.
3.Retrieving the eggs
To collect the egg, a minor surgical procedure “follicular aspiration” is performed. A very thin needle attached with a suction device is inserted through the vagina and into an ovary to suck the eggs out.
4.Insemination and fertilization
The collected eggs are then kept with male sperm under environmentally controlled condition inside a chamber. The sperm enters the egg after a few hours, and the egg gets fertilized, which further divides to become an embryo.
The lining of the womb receives the embryo and for that woman is given progesterone or hCG (human chorionic gonadotrophin).
5.Embryo transfer
With the help of a thin tube (catheter), the embryo is transferred inside the womb through the vagina. A healthy embryo growth can start once the embryo sticks to the lining of the woman’s womb.
An IVF centres or a test tube baby centre like Mohak IVF is an institution upon which you can rely and trust for your needs of becoming parents. We have an excellent reputation in the field of assisted reproductive technology, and we proudly say that we fulfilled many dreams of couples by helping them giving birth to healthy babies.
Mohak Infertility Center is one of the Best Test tube baby centers in indore. This Hospital provide the world class infertility treatment in indore. Dr. Shilpa Bhandari is expert and experienced in male and female infertility treatments. She has to credit her more than thousands of test tube babies and ICSI babies. She has pioneered the advanced techniques in the field of infertility and encouraged the training of IVF specialists by having hand on training workshops of IVF at national and international level. Book an appointment Call now 7898047572 For more information, visit – https://www.mohakivf.com